

Next Lesson - Glomerular Filtration Rate and the Measurement of Kidney Function
Core
A diuretic is a substance that promotes diuresis, i.e. increases urine production. There are many types of diuretics, ranging from everyday substances that cause diuresis to medications that are prescribed to patients if they become fluid overloaded.
- Some examples of substances that cause diuresis which are not diuretics include alcohol, coffee and tea.
- Alcohol inhibits anti-diuretic hormone release and this causes diuresis. See our article on anti-diuretic hormone for more information on how it functions.
- Caffeine causes mild diuresis mainly by reducing sodium reabsorption in the nephron, partly through adenosine receptor antagonism, which reduces water reabsorption.
- Some examples of diuretics include furosemide, bendroflumethiazide, spironolactone and amiloride.
Diuretics act by reducing the reabsorption of sodium (Na) and water in the kidney nephrons. By blocking Na reabsorption, water will not be reabsorbed from the tubules and so will be excreted. Diuretics can either increase or decrease potassium (K) excretion, meaning a patient can become hyper or hypokalaemic depending on the diuretic given.
- Diuretics that cause hyperkalaemia include spironolactone and amiloride.
- Diuretics that cause hypokalaemia include loop and thiazide diuretics.
There are different ways that diuretics work and this depends on the type of diuretic. Diuretics mainly act in the following ways:
- Block Na transporters in the kidney nephron to decrease reabsorption of Na. Diuretics in this category include loop diuretics, thiazide diuretics and potassium sparing diuretics.
- Antagonise aldosterone to reduce its effects and decrease Na reabsorption.spironolactone and eplerenone.
- Osmotic diuretics act by increasing the osmolality of the filtrate in the nephron tubules to stop water being absorbed. The main diuretic in this category is mannitol.
- Inhibition of carbonic anhydrase in the kidney tubules which interferes with the reabsorption of Na and bicarbonate to increase water loss. The main diuretic in this category is acetazolamide.
As diuretics act by increasing water loss, they have two main side effects:
- Hypovolaemia
- Hypotension
When patients are reviewed, these side effects should be looked out for, especially if they are on a high dose of diuretics as that will increase the risk of the patient developing the side effects.
Loop diuretics are the most potent diuretic as they work directly on the loop of Henle where large amounts of Na are reabsorbed.
Loop diuretics work by blocking apical Na-K-Cl2 (NKCC2) transporters in the thick ascending limb of the loop of Henle. By blocking this transporter less Na and chloride (Cl) ions are reabsorbed which decreases the osmolality in the medulla interstitium, and therefore decreases water reabsorption from the descending limb of the loop of Henle. This results in increased water and Na loss from the body.
By blocking NKCC2 transporters, loop diuretics lead to hypocalcaemia and hypomagnesaemia, and so you must watch a patients electrolyte levels to check these do not become too low. Patients develop these low ion levels due to the following steps occurring in the nephron tubules:
- Usually the NKCC2 transporter shifts 2 Cl-, 1 Na+ and 1 K+ into the tubule cell from the nephron lumen. The Na is pumped into the blood using Na-K-ATPase while the Cl drifts back into the blood through its own channel. While this is happening the K drifts back into the lumen through ROMK channels in the apical membrane.
- This movement of K+ ions back into the lumen creates a positive luminal potential that drives the reabsorption of other positively charged ions, like Ca2+ and Mg2+, back into the tubule cells where they can then be moved into the blood.
- When the NKCC2 transporter is blocked this movement of K+ ions stops, and so there is no longer a positive luminal potential which then decreases the reabsorption of the other positively charged ions, resulting in hypocalcaemia and hypomagnesaemia.
Some examples of loop diuretics are furosemide and bumetanide. These two are commonly used in practice for a range of treatments. They have similar side effects and reactions with other drugs.
- Symptoms of Heart Failure - loop diuretics mainly decrease preload, which reduces the symptoms of heart failure but does not have an effect on mortality.
- Acute Pulmonary Oedema
- Fluid Retention - loop diuretics can be used in conditions such as nephrotic syndrome, renal failure and decompensated liver disease if the patient becomes oedematous or is fluid retained.
- Hypertension
- Hypercalcaemia - since loop diuretics impair Ca reabsorption they can be used along with IV fluids, e.g. normal saline, to remove excess Ca.
Side Effects and Drug-Drug Interactions
The side effects that a patient may experience with different loop diuretics are very similar, but there are still some side effects that are different.
As loop diuretics are so potent, the risk of hypovolaemia and hyponatraemia is greater than with other diuretics, so patients on loop diuretics should have their Na level and blood pressure checked every so often, especially if they are on a high dose for a long period of time.
This article will cover the main side effects of furosemide and bumetanide.
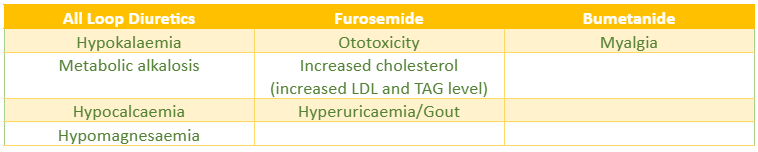
Table - The Side Effects of Loop Diuretics
SimpleMed original by Dr. Thomas Burnell
Drug-drug reactions occur when a patient is taking two or more drugs that interact with each other or have similar effects on the body, resulting in the patient experiencing the side effects of these drugs to a worse severity or making the side effects more likely to occur. The following table demonstrates the main drug interactions that may occur with loop diuretics.
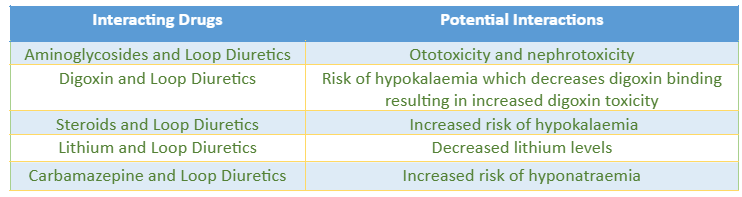
Table - The Main Drug-Drug Interactions for Loop Diuretics
SimpleMed original by Dr. Thomas Burnell
Thiazide diuretics act to increase sodium and water loss by blocking sodium reabsorption in the early distal convoluted tubule (DCT), though it is less potent than loop diuretics.
Thiazide diuretics work by blocking the Na-Cl transporter in the DCT to increase the amount of Na in the nephron lumen. This decreases water reabsorption as there is a higher osmolality in the lumen, preventing water from leaving the lumen causing diuresis.
As thiazide diuretics do not block NKCC2 transporters, calcium handling differs from loop diuretics. Thiazides reduce urinary calcium loss and can increase serum calcium, but they can still cause hypomagnesaemia, so magnesium levels may fall with treatment.
Some examples of thiazide diuretics include bendroflumethiazide, metolazone and indapamide, though indapamide is classified as a thiazide-like diuretic.
- Hypertension - Usually used as the diuretic when treating hypertension
- Nephrotic Syndrome
Side Effects and Drug-Drug Interactions
Thiazide diuretics typically all have the same main side effects and there is not much difference between them. The side effects can be seen in the table below.

Table - The Common Side Effects of Thiazide Diuretics
SimpleMed original by Dr. Thomas Burnell
The common drug-drug interactions involving thiazide diuretics can be seen in the table below.
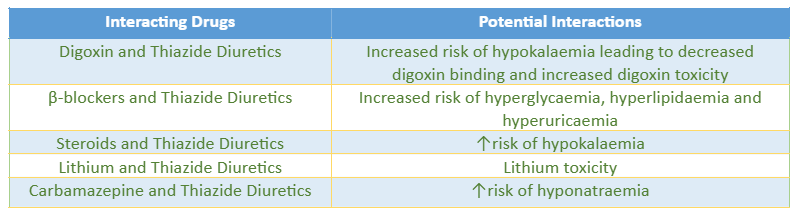
Table - The Main Drug-Drug Interactions for Thiazide Diuretics
SimpleMed original by Dr. Thomas Burnell
Hypokalaemia in Loop Diuretics and Thiazide Diuretics
Both loop and thiazide diuretics have a risk of hypokalaemia because of how they increase the delivery of Na and water to the late distal convoluted tubule and collecting duct. By increasing the delivery of these two substances, potassium excretion into the tubule is affected.
- The increased Na reabsorption by the principal cells of the collecting duct creates a favourable electrical gradient for potassium excretion via apical potassium channels on principal cells.
- The increased amount of sodium and water within the lumen causes there to be a faster flow rate within the tubule. The faster flow rate of the filtrate means K+ ions secreted into the lumen are washed away faster, lowering the K+ ion concentration in the lumen, creating a favourable chemical gradient for K+ ion secretion.
The effect of both of these is increased potassium loss in the urine leading to hypokalaemia.
Aldosterone antagonists work by inhibiting the effects of aldosterone and preventing it’s action on the kidneys. Aldosterone production is stimulated by the Renin-Angiotensin-Aldosterone System and is released from the adrenal cortex. Check out our article on blood pressure for more information about the renin-angiotensin-aldosterone system.
Aldosterone has many effects on the body but mainly acts on the kidneys to increase sodium and water reabsorption. Aldosterone’s functions include:
- Acts on cells in the DCT and collecting duct to upregulate the Na/K pump in the basolateral membrane to create a Na gradient in the cell.
- Upregulates Epithelial Na channels (ENaC) in the collecting duct and colon to increase Na reabsorption and therefore increase water reabsorption.
- Stimulates secretion of K+ ions into the tubule to secrete the excess K brought into the cell by the Na/K pump. The secretion of K also helps to create and maintain the positive luminal potential.
- Upregulates Na/Cl co-transporters in the DCT to increase Na reabsorption.
- Stimulates Na and water retention in the gut, salivary glands and sweat glands to decrease water and Na loss.
Aldosterone antagonists work by inhibiting the functions of aldosterone. By inhibiting epithelial Na channels and Na/K pumps in the DCT and collecting duct, there is a reduction in Na reabsorption resulting in a loss of Na and diuresis.
One of the major side effects of aldosterone antagonists is hyperkalaemia. This happens because the kidneys lose the stimulation to secrete K+ ions into the tubule as aldosterone is being inhibited. Potassium excretion is also decreased because the electrical gradient that promotes K+ ion excretion is reduced because there is a higher concentration of N+ ions in the tubule, increasing the tubule’s positive charge. The potassium level in the body will then rise as it is not removing excess K from the body, resulting in hyperkalaemia.
Potassium sparing diuretics, such as aldosterone antagonists, are usually used in combination with potassium losing diuretics, such as loop diuretics, to reduce the loss of potassium from the body.
The main aldosterone antagonists is spironolactone. This article will be using spironolactone for its uses and side effects of aldosterone antagonists.
- Hypertension
- Heart Failure - the use of spironolactone improves mortality in heart failure
- Decompensated Liver Disease
- Hyperaldosteronism
- Ascites
- Oedema
Side Effects of Spironolactone
All aldosterone antagonists cause hyperkalaemia because they reduce the excretion of K from the body and so the level builds up. The other main side effects of spironolactone are:
- Impotence
- Painful gynaecomastia
Amiloride is a potassium-sparing diuretic that inhibits epithelial Na-channels in the late distal convoluted tubule and collecting duct of the renal nephron to reduce Na reabsorption late on in the tubule, resulting in a small increase in diuresis. Potassium-sparing diuretics have a small diuretic action and cause a small decrease in sodium reabsorption.
Amiloride is known as a potassium-sparing diuretic because it reduces potassium loss from the body. Reduced sodium reabsorption via epithelial Na-channels increases the positive charge in the nephron tubule, resulting in a less favourable electrical gradient for K+ ion secretion into the tubule. Spironolactone is also known as a potassium-sparing diuretic because it reduces K+ ion secretion from the body.
Amiloride is mainly used alongside a potassium-losing diuretic, e.g. loop or thiazide diuretics, to reduce the risk of hypokalaemia.
- Hypertension
- Oedema
- Congestive heart failure
- Ascites due to hepatic cirrhosis
The main side effect of amiloride is hyperkalaemia as this is the main risk of amiloride. Other side effects include:
- Arthralgia
- Decreased appetite
- Nausea and vomiting
- Dysuria
- Dry mouth
Osmotic diuretics function by increasing the osmolality of the blood and the filtrate in the nephron tubule. They are freely filtrated at the glomerulus but are not reabsorbed by the nephron, this means they can increase the osmolality of the renal filtrate, drawing water into the filtrate to decrease water reabsorption and increase water loss from the body. As osmotic diuretics also affect the osmolality of the blood they can be used to draw water out from other parts of the body, e.g. cerebrospinal fluid.
An example of an osmotic diuretic is mannitol. The rest of this article will cover the uses and side effects of mannitol as an example of osmotic diuretics.
Mannitol is used to treat raised intracranial pressure and cerebral oedema. This is because it draws fluid out of the cerebrospinal fluid and brain tissue to decrease the intracranial pressure to relieve the pressure on the brain. It acts by a similar mechanism to draw water out of the brain in cerebral oedema to reduce brain swelling.
Side Effects of Osmotic Diuretics
- Dehydration
- Electrolyte disturbances (e.g. hyponatraemia or hypernatraemia)
- Headache
- Vomiting
- Skin reactions
Carbonic anhydrase inhibitors act by inhibiting carbonic anhydrase, an enzyme found on the apical surface of the tubule cells of the proximal convoluted tubule. The inhibition of this enzyme interferes with the reabsorption of bicarbonate from the filtrate, which inhibits the function of the Na-H exchanger on the apical surface of the tubule cells, reducing sodium reabsorption and therefore reducing water reabsorption causing diuresis.
Examples of carbonic anhydrase inhibitors include dorzolamide and acetazolamide. They are mainly used in the treatment of glaucoma and altitude sickness.
Side Effects of Carbonic Anhydrase Inhibitors
- Renal stones
- Headache
- Eye inflammation
- Vision disorders
- Nausea
As carbonic anhydrase inhibitors inhibit bicarbonate reabsorption, there is an increased risk of acidosis as there are less bicarbonate ions in the blood to react with acid. Acidosis should be looked out for in patients who are on carbonic anhydrase inhibitors as it needs to be treated as soon as possible to avoid further complications.
The following table will give an overview of when diuretics are used and which diuretics are used in each case.
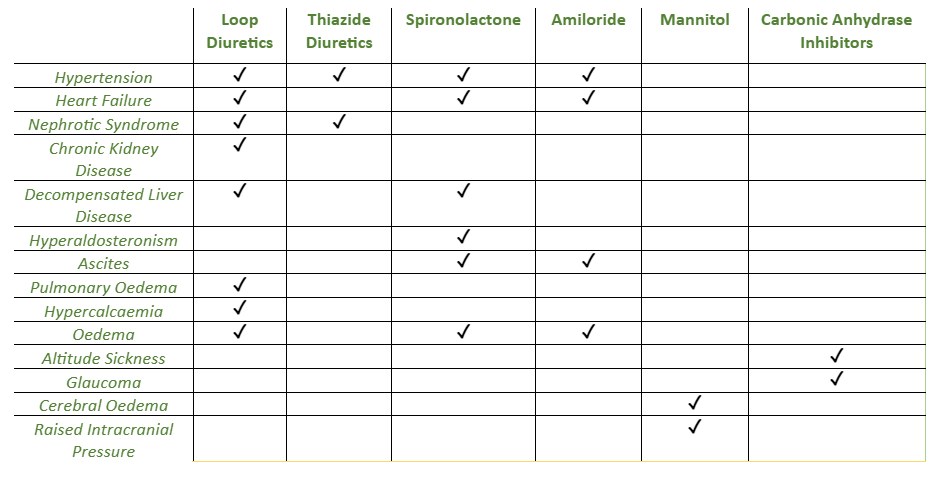
Table - The Main Uses of Diuretics
SimpleMed original by Dr. Thomas Burnell
Edited by: Dr. Maddie Swannack
Reviewed by: Adrian Judge
In this article
Diuretics are substances that promote diuresis. There are lots of different diuretics and they can be drugs or they can be everyday food and drink.
- 640
