

By Dr. Ben Appleby and Dr. Ethan Kavanagh
Next Lesson - Bacterial Structure, Classification and Growth
Core
“Infection models” are usually complex mathematical models used in epidemiology to predict outbreaks of disease and identify solutions to limit damage and exposure via mathematical equations. For the purposes of non-epidemiological specialisation (and this article) the infection model simply models the way in which a patient interacts with a pathogen. This article will also further detail each of the components of each step.
The basic infection model illustrates the pathway a patient travels down from pre-presentation to treatment.
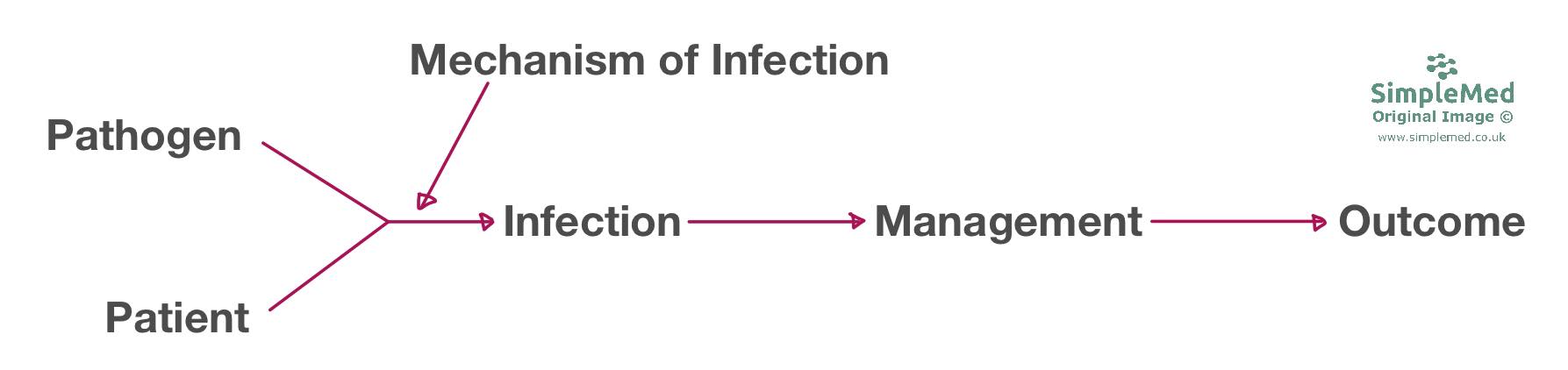
Diagram: The basic infection model, describing the pathway from a healthy patient being infected with a pathogen to their treatment and outcome
SimpleMed original by Dr. Maddie Swannack
Here is a step-by-step run-through of the basic model shown above:
Please note, the rest of the images in this article are courtesy of Dr. D Heney at the University of Leicester Medical School.

The pathogen is the agent that is causing the infection; this could be a virus, bacteria, fungus or parasite. Pathogenesis is the ability of a microorganism to cause disease or morbidity.
Viruses - 2 categories- DNA viruses and RNA viruses
Bacteria - categorised by structure and Gram stain. See our Gram staining and infection investigations article for a full run down.
Fungi:
Yeasts (single cells) e.g. Candida albicans, Cryptococcus neoformans, Pneumocystis jirovecii
Moulds (multicellular) e.g. Aspergillus, Dermatophytes
Parasites:
Protozoa - e.g. Giardia lamblia, Plasmodium falciparum, Trypanosoma cruzi
Helminths - Round worms, flat worms and flukes

The Patient is the uninfected individual who encounters the pathogen and may become infected (also referred to as the susceptible). Their likelihood of infection and susceptibility includes factors about themselves including-
- Age
- Gender (UTIs are much commoner in females due to urethral length)
- Physiological state (overall physical fitness and whether pregnant)
- Pathological state (what current diseases the patient suffers from and any comorbidities e.g. AIDS patients will be immunocompromised and therefore susceptible to opportunistic infection)
- Social factors (quality of housing, food and water quality/safety, IV drug use, sexual partners, proximity of living e.g. Meningitis spreading in university halls previous to the ACWY vaccine.)
Time is considered for two reasons
- Calendar time is important as it is helpful in narrowing down the possible microorganisms the patient has been exposed to at a certain time of the year (seasonal organisms). For example, while the influenza virus can be contracted throughout the year and it is not impossible to get influenza over the summer, it is much less likely to be a differential during summer when a patient presents with respiratory distress. A differential (or differential diagnosis or DDx) is a list of possible conditions which could explain a patient’s condition.
- Relative time is the time between exposure and development of symptoms (incubation period) or the time between the development of additional symptoms.
Place
- Current (hospital or community (i.e. with little to no interaction with healthcare), again relevant in predicting exposure
- Recent travel history (especially relevant in tropical diseases).

Covered in the Introduction to Infection, the mechanisms by which a pathogen can infect the patient are vast.
How a pathogen spreads is incredibly important for determining the potential rate of spread within a population. The rate of spread can be determined using the R0 of a pathogen also known as the basic reproduction number. This figure is a measure of the transmission potential of a disease and is defined by the number of secondary infections produced by a typical case of an infection in a population that is totally susceptible. Put simply, this describes how many additional people are infected by each infected patient. For example, if the R0=2 then for every patient infected with the disease, they will pass on the infection to two other uninfected individuals - this will of course lead to an overall increase in number of cases. The figure is determined by the pathogen’s mechanism of infection and ability to live within a host while that host is able to further transmit the infection.

Management is usually the first step in which a medical professional is usually involved. It starts with the establishment of a diagnosis where possible (using data collected from the history-taking process, examinations and investigations) and is followed by the treatment course administered for that infection. Treatment is usually empirical - targeting the most likely cause of infection even if it has not been confirmed via bacteriology i.e. microscopy, culture and susceptibility testing (M,C and S)

There are two broad types of treatment: specific and supportive
Specific treatment focuses on treating the underlying cause of a disease. For an infectious disease this involves giving antibiotics/antivirals which the pathogen is known to be susceptible to.
Alongside antimicrobials, in some cases surgery can also be used to treat an infection:
- Drainage may be used in cases where there may be a large amount of pus e.g. in an infected ulcer. By draining the ulcer, the bacterial load can be reduced and give the patient’s immune system a better chance of clearing the infection.
- Debridement refers to the removal of infected/damaged/dead tissue. Again, this helps aid the healing of the surrounding healthy tissue by reducing bacterial load and removing unsalvageable tissue which may lead to further complications if not removed. Debridement may be carried out by surgical excision or by other means including maggot therapy.
- Dead space removal involves removing an empty area that infection may move into (possibly created by debridement) thus stopping the spread/dissemination of an infection. This may be as simple as using antibiotic coated swabs to physically block off and occupy dead space.
Supportive treatment is aimed at treating the symptoms of a disease, lessening the impact of the side effects of treatment and overall improving patient comfort.

Infection prevention involves stopping an infection spreading from one patient to another in a clinical or community setting. The 4 main areas of infection prevention can be remembered as the 4 P’s:
- Patient- minimise patients' risk factors for infection by optimising health and controlling interaction with visitors and other patients e.g. by isolation in side rooms/ negative pressure rooms. This may also include the use of prophylactic antibiotics in immunosuppressed patients e.g. Asplenic patients.
- Pathogen - prevent the pathogen from causing infections. This can be achieved by minimising inappropriate antibiotic use to limit resistance and ensuring good levels of vaccination within the general population. Healthcare workers should also be fully vaccinated and healthy.
- Practice- modify healthcare worker activity to prevent iatrogenic spread of disease. This includes effective hand hygiene and professional dress standards including the policy ‘bare below the elbow’ preventing long sleeves, watches, jewellery etc from harbouring and spreading germs. This is also bolstered by a member of staff on each ward designated to making sure rules are followed to prevent any spread or outbreaks (this person is typically an infection control nurse). The Health and Social Care Act 2008 has a page outlining the infection control protocols GP practices and the NHS etc have to follow:
- Place- this includes the environment in which the patient is in and the equipment used. This includes sterilisation and disinfection of equipment and the ward environment to eliminate reservoirs of infection.
In the community, the main ways to prevent infections are avoiding risk factors, immunisation and prophylaxis (preventative treatment) linked with contact tracing.
An example of avoiding risk factors would be a child with chicken pox (Varicella zoster), who would be kept away from other susceptible individuals (those who have previously had Varicella become immune after their first exposure and so are no longer susceptible).
Contact tracing and prophylaxis are used in the instance of notifiable diseases (diseases which if suspected require reporting to the UK Health Security Agency to prevent outbreaks or any further spread). Contact tracing involves finding out who the patient has recently interacted with and providing them with prophylactic treatment to prevent them for developing and spreading the disease.
Vaccines operate on the concept of herd immunity. Immunising one individual removes them from the pool of susceptible individuals who may catch the pathogen. If enough people are vaccinated ("the herd"), then the microorganism does not have enough susceptible people to move to in the time in which it is infective within an individual. This concept also helps protect those who cannot be immunised including; immunosuppressed individuals and children who are too young to be immunised The NHS in the UK runs a full immunisation programme - here is a full list of what the NHS provides to children.
Healthcare acquired infection (HAI)
For an infection to be classed as healthcare acquired rather than community acquired, the infection must have been neither present nor incubating on admission. In practice, infections that develop more than 48 hours after admission are commonly classed as HAIs. HAIs should be avoided due to the impact on the health of the patient as they may possibly worsen the condition or lead to complications and the increased cost of a prolonged stay and use of a bed.

Outcome describes the final condition of the patient post-infection. Outcome is a spectrum ranging from complete cure to death with chronic infection/long-term morbidity/disability in between.
Edited by: Dr. Marcus Judge and Dr. Ben Appleby
In this article
In this context an infection model is a graphical representation of the different components involved in an infection “Infection models” are usually…
- 11042
