

Next Lesson - Basics of Bone Anatomy
Core
This article describes the structure of bones from a molecular perspective. More information can be found on the anatomical relationships of bones in the rest of our Musculoskeletal Section.
The skeleton in an adult human is made up of 206 bones and facilitates the movement of the body and the protection of important internal organs.
See our article ‘Basics of Bone Anatomy’ which includes information about the types of bones and their functions.
There are three main types of cell that make up bone tissue.
Osteoblasts are derived from mesenchymal stem cells and are responsible for the laying down of bone. This is done through the production of dense collagen and hydroxyapatite (the mineral component of bone). Osteoblasts are closely associated with one another, forming an osteon. Once the osteoblast has surrounded itself with bone matrix, it becomes trapped in its lacuna and becomes an osteocyte.
Osteocytes are star-shaped cells that cannot divide. Osteocytes are formed from osteoclasts that have been trapped in the bony matrix that they have secreted and exist in a space called a lacuna. This restrictive space means that the osteocytes are no longer able to produce osteoid (bone tissue). The processes of an osteocyte instead stretch out, connecting to other osteocytes through canaliculi.
Osteoclasts are the type of bone cell responsible for the break down of bone tissue through the release of acid (to dissolve the hydroxyapatite crystals) and collagenase. They have an important role in remodelling of bone and regulation of calcium levels in the blood, but also play a key part in the pathophysiology of osteoporosis. The osteoclasts originate from haemopoietic stem cells, rather than mesenchymal stem cells which produce osteoblasts.
There are two types of bone tissue namely compact (cortical) bone and spongy (trabecular) bone.
The main building block of bone is an osteon, shown in the image below. It is a collection of osteocytes trapped in the bone matrix that they have secreted. The individual osteocytes communicate with each other through microscopic canals called canaliculi. An osteon has a central canal called a Haversian Canal, which contains blood vessels and nerves to supply the bone.![]()
Image: this diagram shows the structure of an osteon; note the Haversian canal and the lamellae created by osteocytes.
Source: https://en.wikipedia.org/wiki/Osteocyte#/media/File:Transverse_section_of_bone_en.svg
Compact bone consists of closely packed osteons. An osteon is made up of a central canal called the Haversian canal, surrounded by concentric rings of matrix called lamellae. These Haversian canals lie parallel to the axis of the long bone.
Between the lamellae are osteocytes, mature bone cells which have been surrounded by bony tissue and now exist in lacunae. The lacunae are connected by canaliculi.
Smaller canals known as perforating or Volkmann’s canals connect the Haversian canals to provide passageways through the hard matrix. They run at 90 degrees to the Haversian canals, across the width of the long bone.
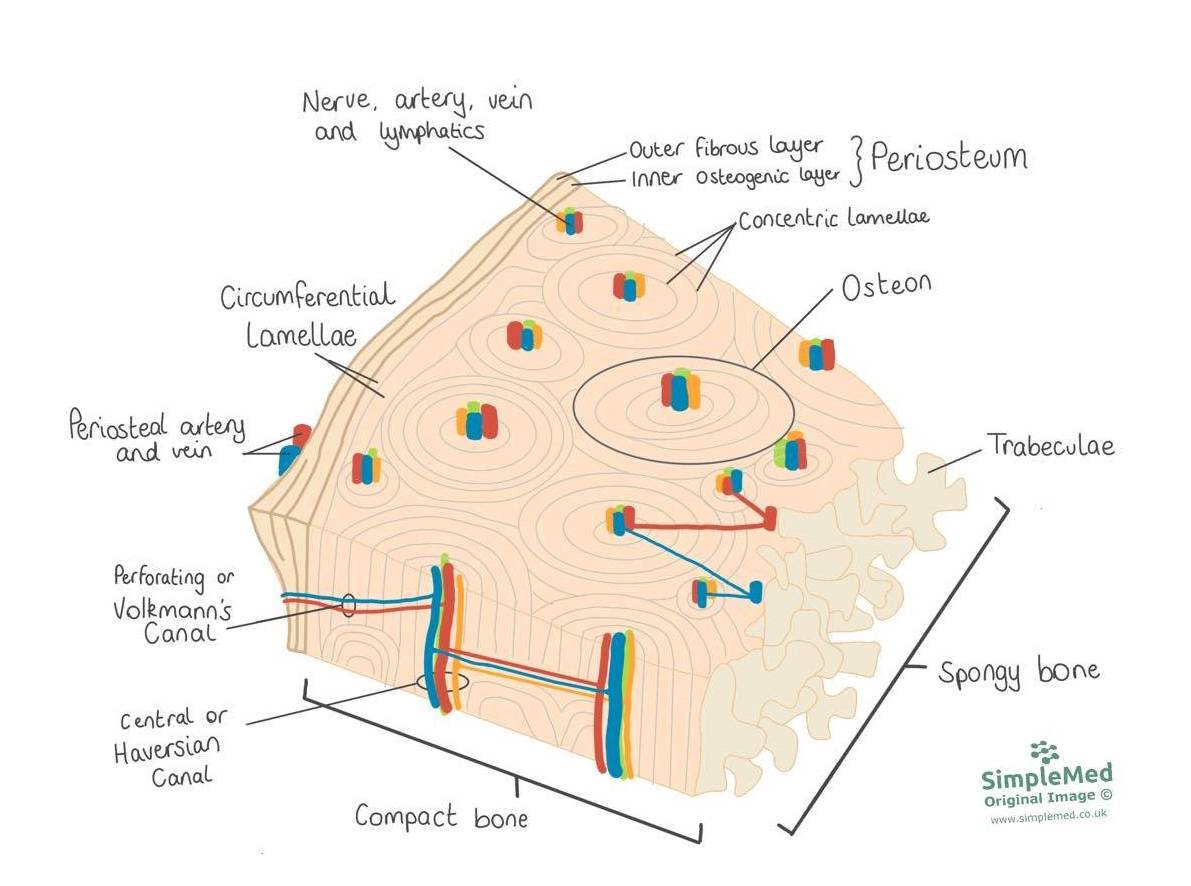
Image: this diagram shows the structure of a long bone. Key features include the periosteum, the lamellae of the osteons and the trabeculae of the spongy bone centre.
SimpleMed original by Dr. Maddie Swannack
Spongy or cancellous bone is lighter and less dense than compact bone. It consists of plates called trabeculae, bars of compact bone, and irregular cavities that contain red bone marrow (responsible for haematopoiesis). While it may seem that the trabeculae are arranged randomly, in fact they are organised to provide maximum support. They are aligned along the stress points of the bone and can realign if the direction of the stress on the bone changes.
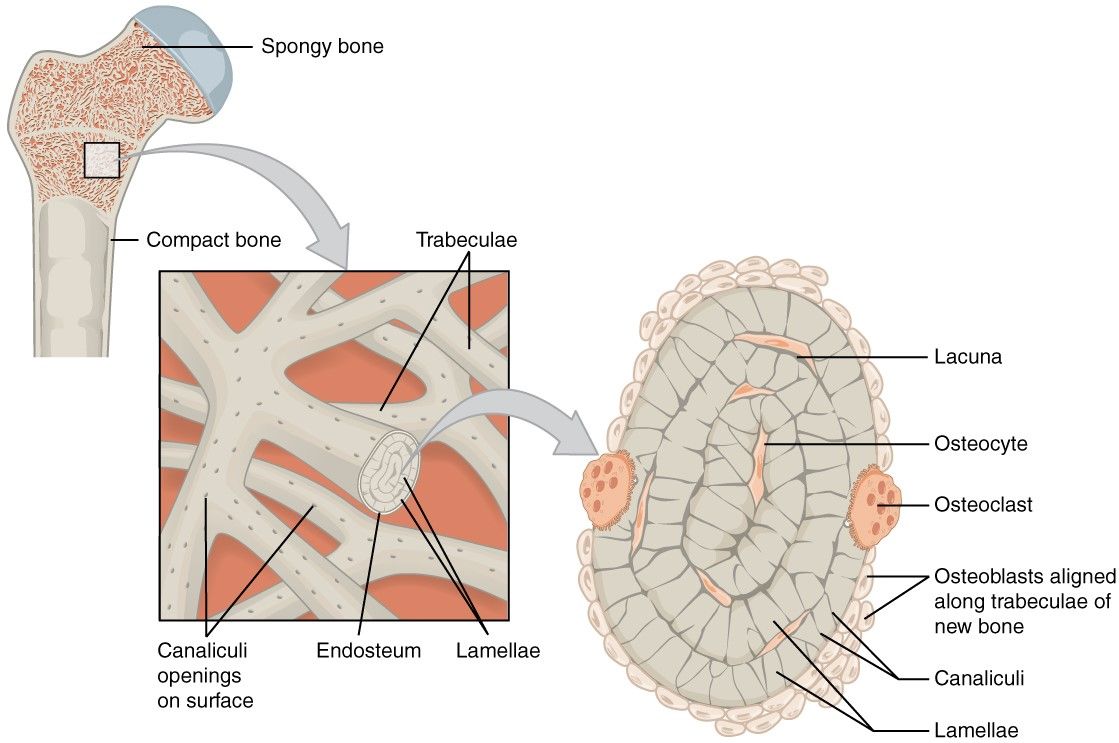
Image: this diagram shows the structure of spongy bone, highlighting the trabeculae and marrow spaces within cancellous bone.
Source: https://commons.wikimedia.org/wiki/File:606_Spongy_Bone_esp.jpg
In the body there are two mechanisms through which bones are created.
The first, endochondral ossification, involves converting a cartilage template into bone. The second, intra-membranous ossification, involves the production of bone from stem cells without a cartilage template. Endochondral ossification is responsible for the lengthening of long bones through growth at epiphyseal growth plates.
Endochondral ossification produces long bones from a cartilaginous template.
The stages are shown in the following diagram:
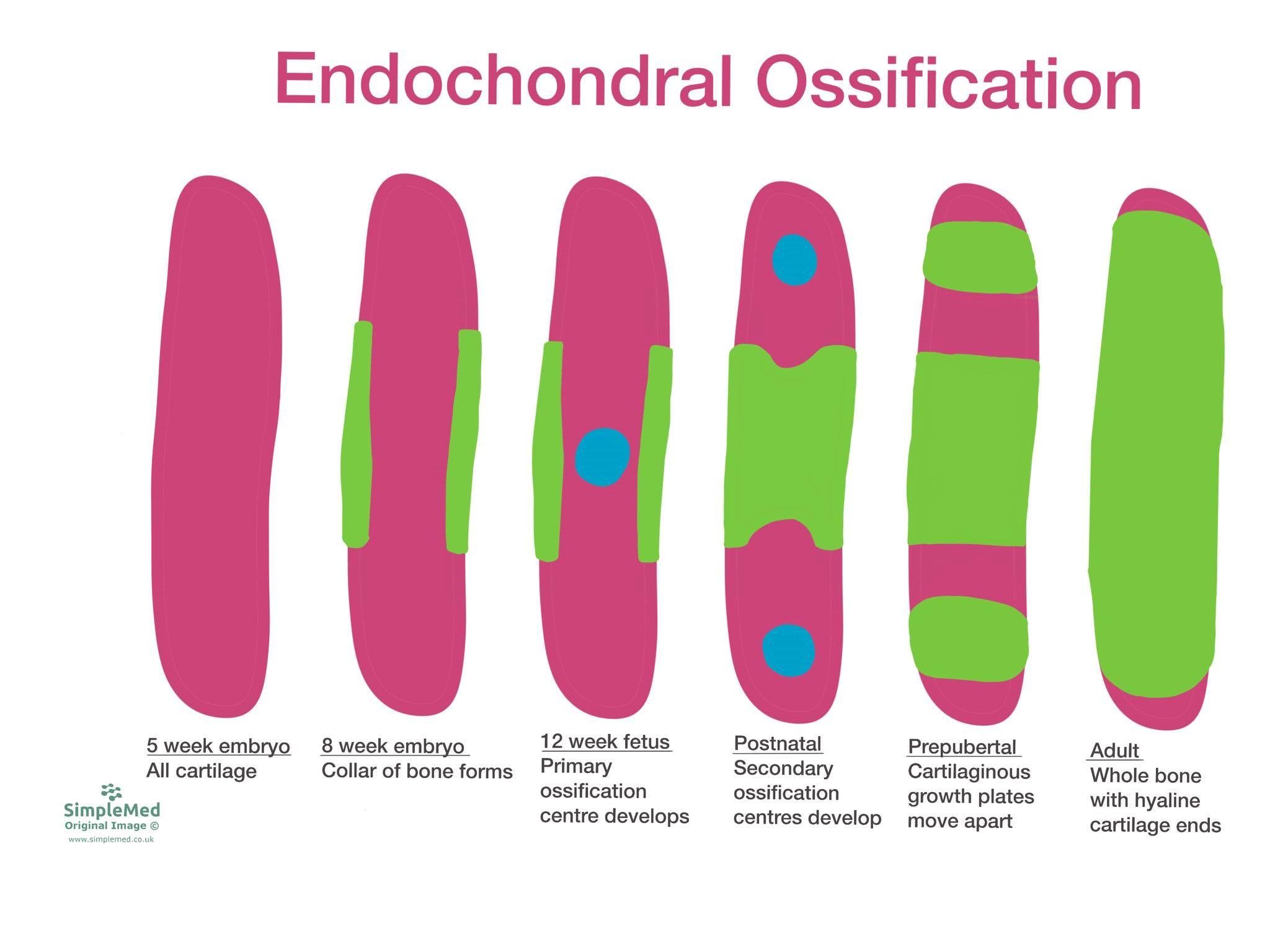
Image: this diagram shows the development of a long bone from cartilaginous template through endochondral ossification. In this diagram, pink represents cartilage, green represents bone and blue represents an ossification centre.
SimpleMed original by Dr. Maddie Swannack
Endochondral ossification begins at around 5 weeks gestation, when the long bones have a complete cartilaginous template formed. Around 3 weeks later, a collar of bone begins to form around the middle of the bone.
At 12 weeks gestation, the primary ossification centre of the bone develops. From this point, the development of bone spreads out from the primary ossification centre until the middle of the bone is complete.
At birth, the secondary ossification centres have developed at the ends of the bone and over childhood these develop into bone themselves, leaving cartilage in two sections: at the end of the bones to lubricate the movement of the bones, and in stripes slightly medially in the bone to allow the growth of the bone. These stripes are called epiphyseal growth plates.
As an adult, when full length of the bone has been achieved, the epiphyseal growth plates fuse and leave only the ends capped with cartilage.
The stages of intramembranous ossification are as follows:
- Mesenchymal stem cells form an ossification centre and differentiate into osteoblasts, which begin to lay down osteoid (bone tissue).
- Rudimentary bone forms as bony spicules, surrounded by functional osteoblasts and containing osteocytes.
- These bony spicules are remodelled into trabeculae, which eventually are replaced by the lamellae of compact bone.
Osteoporosis is a disease that involves a mismatch between osteoblast and osteoclast action, with bone breakdown being much faster than bone creation. This causes a decrease in bone mineral density, leading to an increased risk of fractures.
Fractures are the main symptom of osteoporosis, with common sites of fracture being vertebral bodies, femoral neck, radius and ulna. These fractures can occur with a comparatively small amount of force due to the decreased density of bone. Complications of such fractures can include chronic pain and decreased mobility.
Risk factors for osteoporosis include:
- Menopause - oestrogen is a protective factor for osteoporosis, meaning that decreased levels of oestrogen experienced after menopause increase the risk of osteoporosis.
- Chronic kidney disease - the diseased kidneys are unable to properly regulate levels of minerals in the body, which makes laying down bone more difficult.
- Medications such as corticosteroids - steroid use increases osteoclast action and affects calcium excretion (which makes creating bone more difficult).
- Smoking and inactivity.
- Increased age.
A healthy balanced diet throughout life and reducing use of medications that increase the rate of bone loss is key to preventing osteoporosis.
Prevention of fractures in a patient who has established osteoporosis can be done through improving diet, increasing exercise, stopping smoking, reducing alcohol and preventing falls.
Bisphosphonate containing medications are useful in patients with osteoporosis to decrease the occurrence of future fractures.
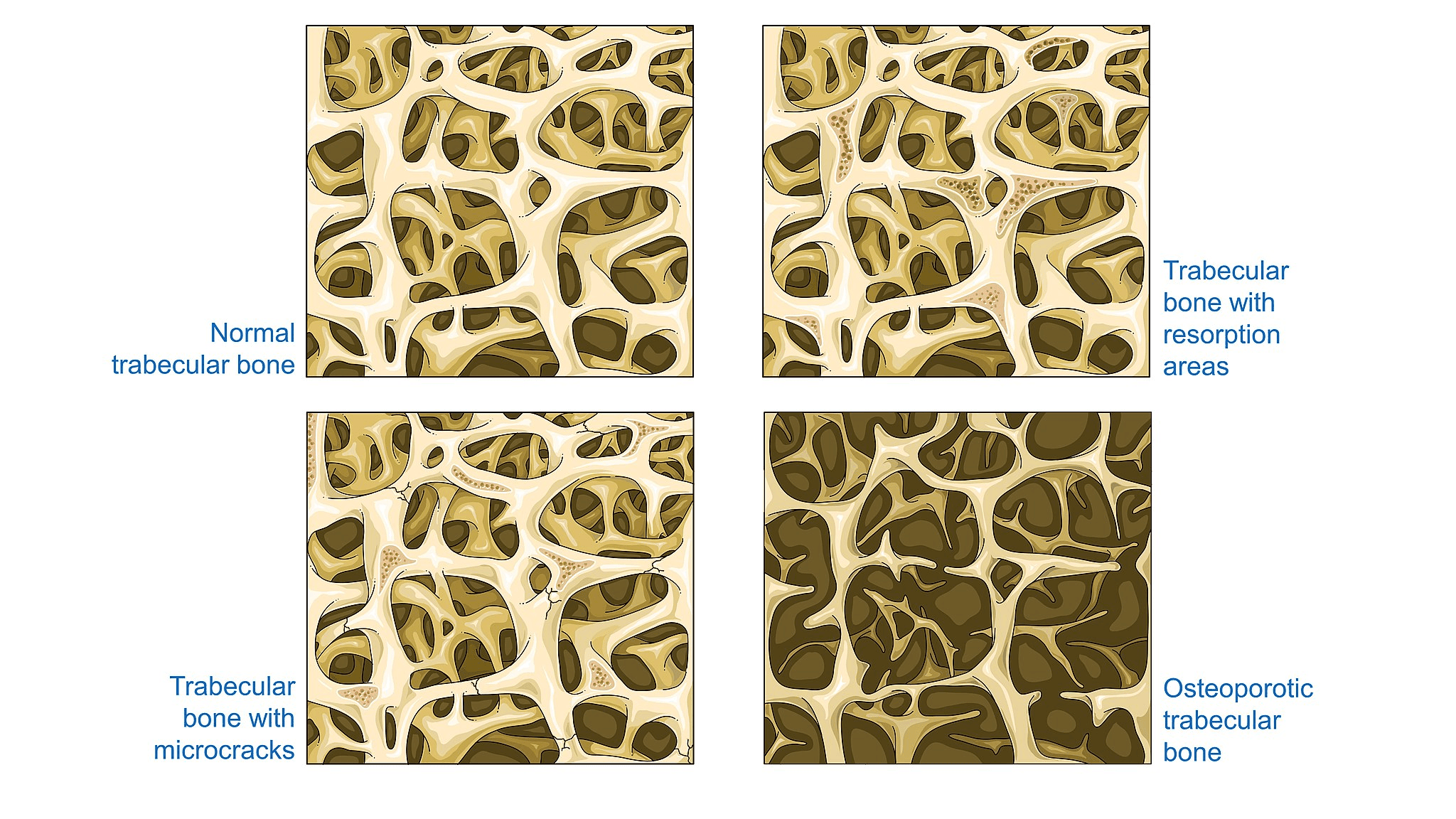
Image: this diagram shows the stages of bone condition leading to osteoporosis.
Source: Laboratoires Servier / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)
Fractures of bone occur when the periosteum is disrupted. Fractures require significant force in the young, but less force in the elderly due to the higher incidence of osteoporosis in this age group.
One important consideration when assessing the severity of a fracture is whether the fracture is open or closed. An open fracture is one that has broken the skin usually due to a fragment of bone protruding through the skin. This is clinically important as a break in the skin provides a route into the bone for infection.
Another consideration is whether a fracture is complete (all the way through the bone) or partial (only including one side of the periosteum).
There are six classifications of types of fractures:
- Transverse - a fracture which may be caused by forces pressing on both ends of a bone or more commonly by force from the side.
- Spiral - a fracture that spirals round the periosteum, caused by a twisting force.
- Comminuted - a fracture that involves many pieces of bone.
- Impacted - a fracture caused by a force on one end of the bone.
- Greenstick - a fracture occurring mostly in children due to the immaturity of the periosteum, caused by forces that bend the bone.
- Oblique - a fracture that crosses the bone in a diagonal direction.
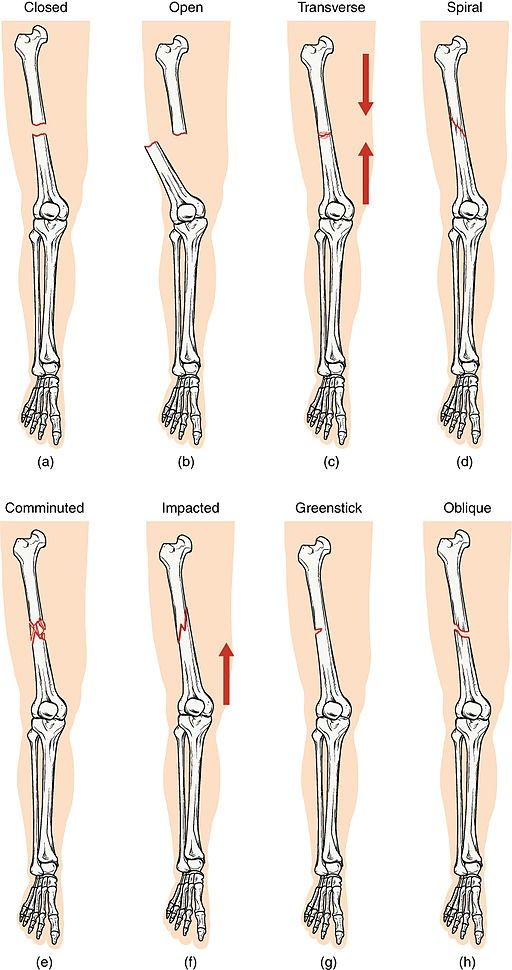
Image: this diagram shows the different types of fractures.
Source: OpenStax College / CC BY (https://creativecommons.org/licenses/by/4.0)
There are two types of fracture healing depending on the conditions of the break and the repair.
Primary intention healing occurs when two ends of bone are fixed together surgically with absolute stability, so the fracture site is held under compression. This means that the osteoclasts and osteoblasts don't realise there is a fracture at all, and continue the build-break cycle as normal. This heals the bone without the need for callus formation.
Secondary intention healing occurs when there is not significant tension on the bones, basically any fracture that is not operated on. This type of healing follows the stages below, which are important to know to understand the management of fractures. The stages of repair are as follows:
- A haematoma forms due to the interruption of blood vessels within the bone causing swelling.
- New blood vessels permeate the haematoma, forming a pro-callus of granulation tissue.
- Fibroblasts and chondroblasts produce cartilage.
- Osteoblasts begin to work, forming the soft callus.
- Trabeculae form through endochondral ossification, producing the hard callus.
- Lamellae bone forms and remodelling by osteoclasts
It is important that the bone is protected and immobilised until the hard callus forms, so that no further damage occurs. In any plaster or support it is also important to allow space for swelling to form and recede without restriction. This can be achieved by allowing space in a cast, or by replacing casts.
Remembering the stages of fracture repair can be very difficult. A mnemonic can be helpful, and one that I use is:
Herds of Haematoma
Giraffes Granuloma (and angiogenesis)
Stampede Soft callus
Hiroshima for Hard callus
Lovely Lamellae bone formation
Radiation Remodelling
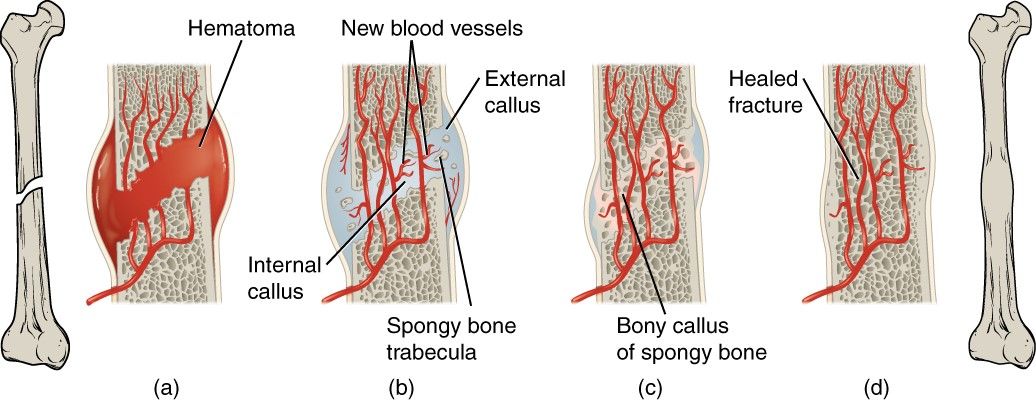
Image: this diagram shows a simplified version of the stages of fracture repair. In this image, the label of external callus represents the soft callus as at this point it only contains soft tissue.
Source: OpenStax College / CC BY (https://creativecommons.org/licenses/by/3.0)
Edited by: Dr. Ben Appleby
Reviewed by: Dr. Marcus Judge
In this article
There are 206 bones in the adult body. The functions of bones include locomotion, protection and haematopoiesis to name a few.
- 11631

{kind=link}
{kind=link}