

By Dr. Maddie Swannack and Dr. Ben Appleby
Next Lesson - Muscles in Action
Core
In this article, there are many names used for muscle cells: ‘myocyte’, ‘muscle fibre’, and ‘muscle cell’ all mean the same thing. They have different names because it can be easier to picture if the cell is described as a ‘fibre’ or ‘filament’ rather than a ‘cell’, but they all mean the same thing.
There are three main types of muscle in the body:
This type of muscle is what is called ‘muscle’ by the public. It is the muscle that makes up triceps and quadriceps, is used to move the skeleton about, and that can be built up through things like weight training.
Skeletal muscle cells are very long, with one cell (one muscle fibre) stretching the whole length of the muscle, which can be up to 30cm. Because they can be so long, they need to have multiple nuclei, so there are multiple copies of the genes needed to code for proteins.

This image shows skeletal muscle cells. Note the long cells, the multiple nuclei per cell and the striations visible.
Creative Commons Source Nenad Bursac, Ph.D., Duke University
This type of muscle is found only in the heart. The muscle cells found here are specially adapted to contract rhythmically and without pausing: they have many mitochondria. They are most commonly mononucleated (meaning they have only one nucleus) and are not as long as cells found in skeletal muscle. Other than only having one nucleus per cell, and not being as long, cardiac muscle cells are visually very similar to skeletal muscle cells.
An important feature of cardiac muscle is that it releases chemicals depending on its state:
When cardiac muscle cells are damaged, like in ischaemia caused by a heart attack, they release troponin, a molecule used to regulate contraction (see later - actin and myosin). This means that troponin assays can be used to check for myocardial cell damage.
If cardiac muscle cells are stretched but still have intact cell membranes (called sarcolemma), like in heart failure, they release Natriuretic Peptides. These proteins decrease blood volume and vascular resistance to decrease the amount of stretch on the heart, which reduces the amount of stress the heart is under. In atrial distension, Atrial Natriuretic Peptide is released (ANP), as seen in mitral valve stenosis. With ventricular distension, Brain Natriuretic Peptide is released (BNP), as seen in heart failure. This is a misnomer, it is named ‘brain’ because it was first isolated in brain tissue, but it is released from the ventricular wall.
This type of muscle is used for unconscious mechanisms in the body, like digestion and continence. It is found in the walls of arteries, the small intestine and the pelvic floor, and is not under conscious control.
Smooth muscle is different in structure to other types of muscle. It doesn’t have the organised sarcomeres like cardiac and skeletal (meaning it is not striated), and does not have T tubules in the sarcolemma.
The actin-myosin interactions that occur in smooth muscle are slow and sustained, with a low ATP demand. This is good because it allows the maintenance of muscle contraction over a long period of time, which is useful for things like sphincters that maintain continence.
Smooth muscle cells can respond to nerve impulses like all forms of muscle cells, but can also respond to hormones, drugs and gases dissolved in the blood.
Smooth muscle cells also play a vital role in the pathophysiology of some diseases: in asthma, it is a contraction of the smooth muscle cells in the bronchi which constricts the airways.
Modified types of smooth muscle cell can have other functions as well as contraction: myoepithelial cells can form a basketwork around secretory units and contract to cause secretion, and myofibroblasts produce a collagen-containing matrix which can contract.
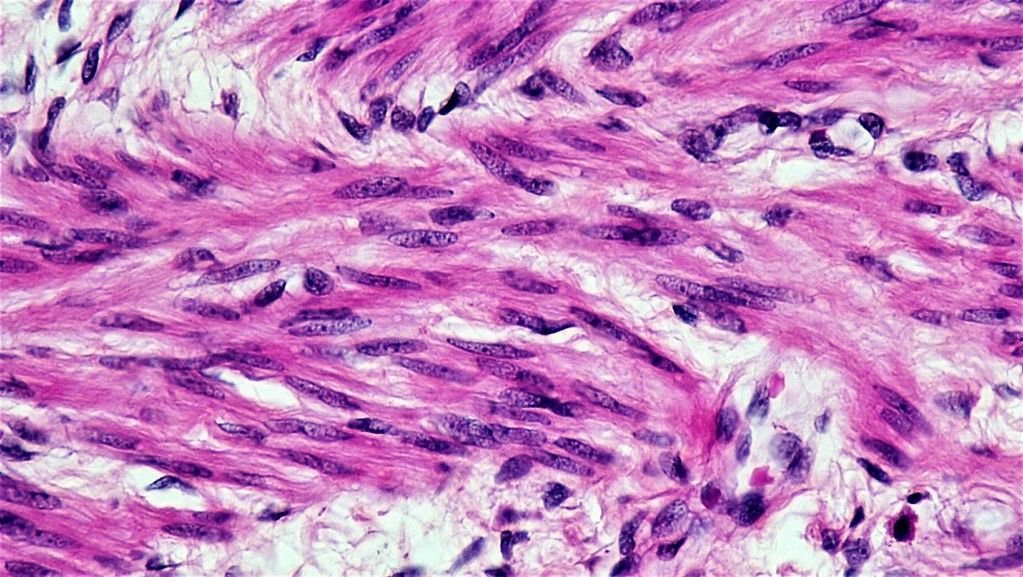
This image shows smooth muscle cells. Note their lack of striations (stripes), which shows there are no organised sarcomeres, and the spindle shapes of the cells.
Public Domain Image Source
Muscles are made up of many layers of fibres that are organised into bundles. The diagram below shows how each muscle fibre is wrapped in a layer of endomysium (connective tissue). These fibres are collected together into a bunch, called a fascicle. This fascicle is wrapped in perimysium. A number of fascicles are then collected together, with blood vessels, into a layer of epimysium, which forms the muscle as a whole.
![]()
This diagram shows the transverse section of a muscle, showing the layers of connective tissue in purple (epimysium), green (perimysium) and orange (endomysium).
SimpleMed Original by Dr. Maddie Swannack
In summary:
- Muscle fibres are wrapped in endomysium.
- Multiple muscle fibres are collected and wrapped in perimysium and become a fascicle.
- Multiple fascicles are collected along with blood vessels, and wrapped in epimysium, becoming the muscle itself.
This can be a complicated thing to understand, but when remembering the order of the connective tissue layers, remember that ‘endo-’ means inner, ‘epi-’ means outer, and ‘peri-’ is the one in the middle.
A muscle cell, or fibre, is made up of multiple different filaments. The main two of these are called myosin and actin. Myosin is also known as the thick filament, because as shown in the diagram below, it has many strands and many heads. These heads connect with the actin filaments (also shown below) which are called the thin filaments. Together they make up the sarcomere.
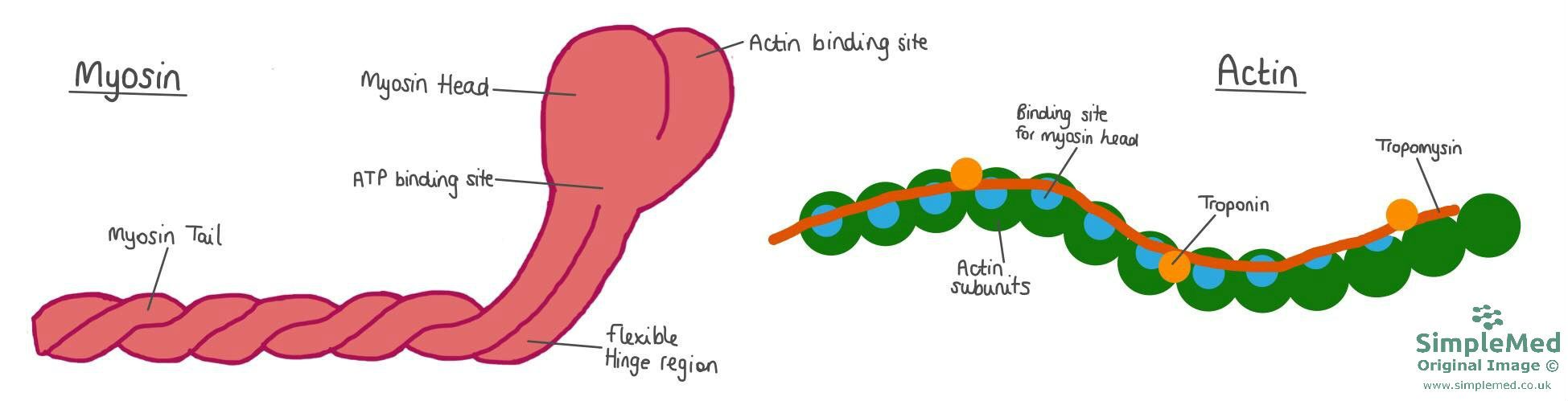
This image shows one molecule each of actin and myosin. Note the different parts associated with the actin filament (troponin and tropomyosin) and how they block the binding sites for the myosin heads.
SimpleMed Original by Dr. Maddie Swannack

This image shows the thin and thick filaments. The thick filament has many myosin in it, meaning it has many heads to create strong bonds with the thin filament.
SimpleMed original by Dr. Maddie Swannack
The thin filament is often referred to as actin alone, despite the fact it is made up of more than one type of molecule. The thin filament is made up of actin, troponin and tropomyosin. Troponin is important because it can be used as an indicator of cardiac muscle damage (eg in a heart attack). This is possible because the type of troponin is specific to the type of muscle, so troponin assays used to look for cardiac damage are only looking for that type of troponin.
It is important to note however, that smooth muscle does NOT contain troponin, but instead uses a protein called calmodulin. Calcium binding to calmodulin leads to activation of enzymes that allow myosin to interact with actin, rather than moving a blocking protein on actin as occurs with troponin in striated muscle.
The sarcomere is the name for the portion of the muscle fibre from Z line to Z line. This is quite a complicated definition to start with, but it is important to know the definition. It will make more sense in a minute.
The easiest place to start is the A band. This is the area of the sarcomere where myosin is present. Because myosin is thicker, the A band is darker (dArker is the A band).
Because of the overlapping present between actin and myosin, there is a portion of the A band that does have actin present, and there is a portion that does not. This area that does not have actin on it (only myosin) is called the H zone. This area becomes especially important later when considering the sliding filament theory (see below). Because there is no actin present in the H zone, there are no myosin heads here, because they would have nothing to attach to. The centre of the H zone is called the M line. The M line is the centre of the sarcomere.
The other portion of the sarcomere is called the I band. This is the portion of the sarcomere that contains only actin (as in there is no myosin here at all). Because this part of the sarcomere has only the actin, which is the thin filament, it makes this area much lighter on images (lighter is the I band). The centre of the I band is called the Z line, the line that was mentioned earlier as the edge of the sarcomere.
In summary:
- M line is the centre of the H zone.
- H zone is the portion of the A band that does not have actin present (only myosin).
- A band is any portion of the sarcomere with myosin in it.
- Z line is the centre of the I band.
- I band is the portion of the sarcomere with only actin present.
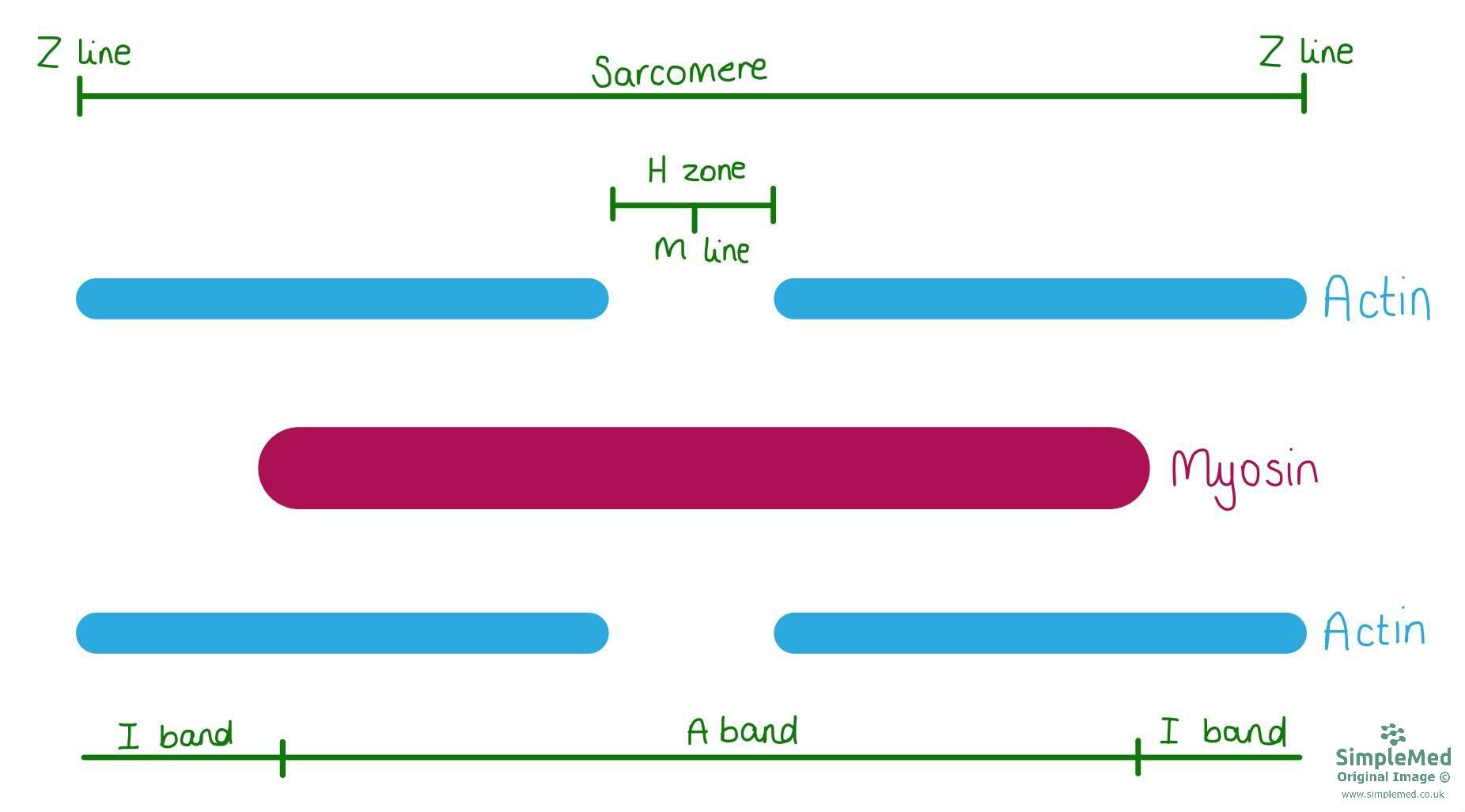
The zones and bands of the sarcomere.
SimpleMed Original by Dr. Maddie Swannack
The image above shows the sarcomere, the relationship between the thick and thin filaments. It shows the different regions of the sarcomere in an attempt to make the complicated names easier to understand.
It is important to remember that it is the sarcomere that gives striated muscle (skeletal and cardiac) the stripy pattern. While smooth muscle cells do contain actin and myosin, they are disorganised, meaning the stripes caused by the sarcomere organisation do not occur.
So a muscle cell is made up of many sarcomeres arranged end to end, forming myofibrils. However, muscle cells need certain other things to survive just like any other eukaryotic cell.
Mitochondria are spread throughout the muscle cell, being able to provide the ATP needed for muscle contraction.
Each muscle fibre is wrapped in the connective tissue layer of endomysium, but it also has a cell membrane that performs all the normal functions of a cell membrane. This is called the sarcolemma. Because it is important that the surface area of the sarcolemma is large (so action potentials that arrive at the neuromuscular junction can be detected and quickly result in a contraction), the sarcolemma folds itself into deep valleys called T tubules. These allow for rapid muscle contraction with increased surface area, and so only the sarcolemma on cardiac and skeletal muscle needs T tubules (smooth muscle still has sarcolemma).
Cytoplasm in the muscle cell also has a special name: sarcoplasm. This is the same as the cytoplasm of any other cell, except it contains a lot of glycogen stores, and a molecule called myoglobin (an oxygen carrying molecule similar to haemoglobin, but made of only one protein and with a very high affinity for oxygen). For more information on myoglobin, see our Protein Function in Oxygen Transport article.
Another key part of a muscle cell is the sarcoplasmic reticulum (SR), a specialised form of smooth endoplasmic reticulum found in myocytes.
The SR extends through and around the muscle fibres, and its main function is to store and release calcium. This is important because at rest, the tropomyosin sits over the sites on the actin where the myosin heads are supposed to bind, so the muscle would be unable to contract through sliding filament theory (see below). It is through the release of the calcium by the SR that the tropomyosin moves, and the myosin head can actually bind to the actin.
The steps for the calcium release from the SR are as follows:
- Nerve impulse arrives at the neuromuscular junction
- Acetylcholine is released into the synaptic cleft, causing post-synaptic opening of sodium channels.
- Depolarisation spreads over the sarcolemma and through the T tubules.
- Voltage sensitive proteins inside the T tubules change conformation.
- This opens the gated calcium channels, meaning calcium is released into the sarcoplasm from the SR.
- Calcium binds to the troponin (subunit TnC), moving the troponin and tropomyosin away from the myosin binding site, and allowing the interaction to occur.
Following this, sliding filament theory occurs, allowing muscle contraction.
Sliding filament theory describes how actin and myosin interact to produce muscle contraction. It has four stages:
- The myosin heads form a cross bridge with the actin filament.
- The attached heads pull on the actin filament in a power stroke, an active process driven by changes in the myosin head.
- ATP attaches to the myosin head, and this breaks the bond with the actin filament.
- The ATP hydrolyses and ‘cocks’ the myosin head back to the starting position (active movement).
This movement slides the myosin filaments along the actin, causing the I band to shrink as the overlap increases.
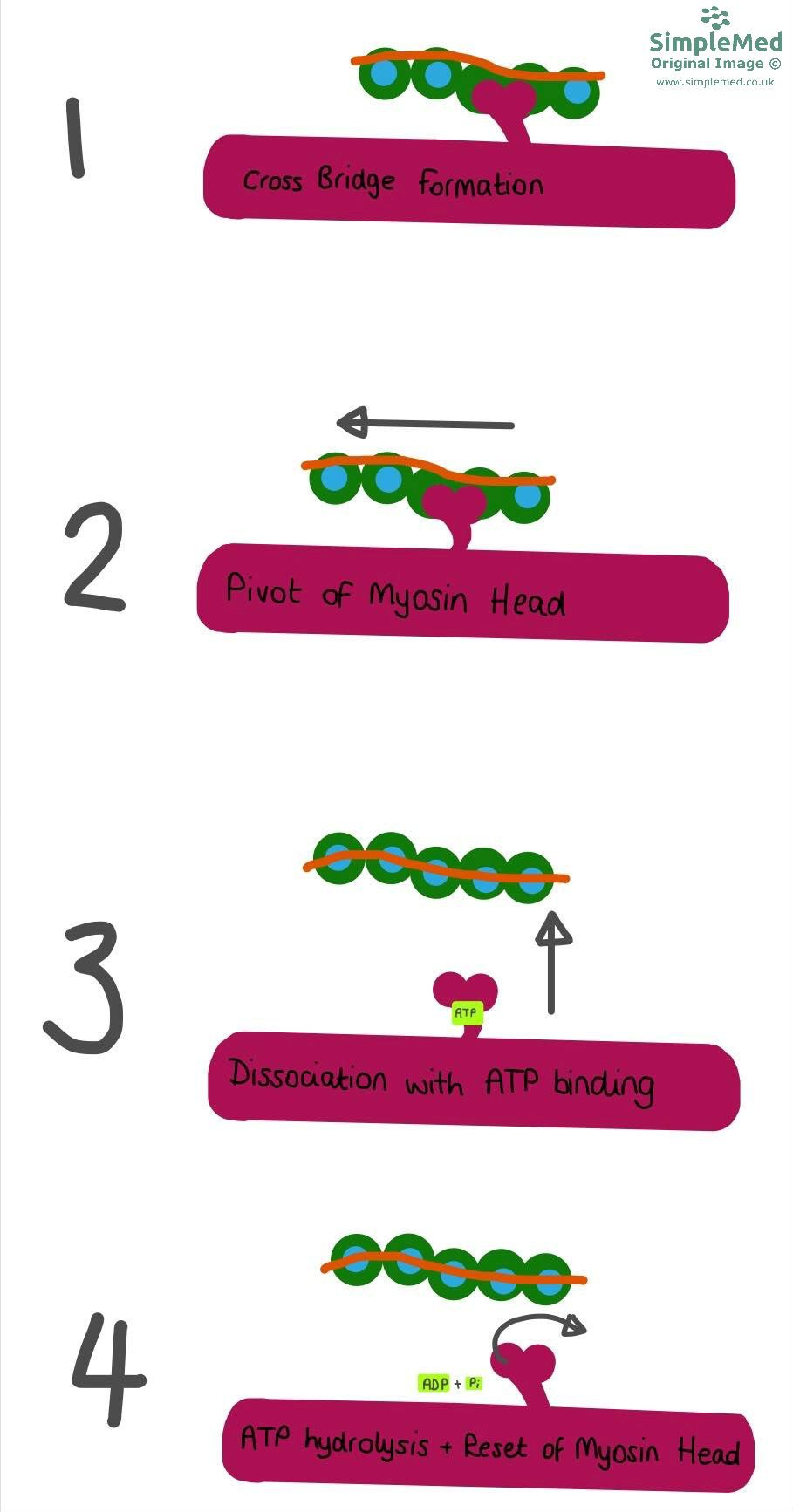
This image shows the four stages that take place in the Sliding Filament theory, explained above the image.
SimpleMed original by Dr. Maddie Swannack
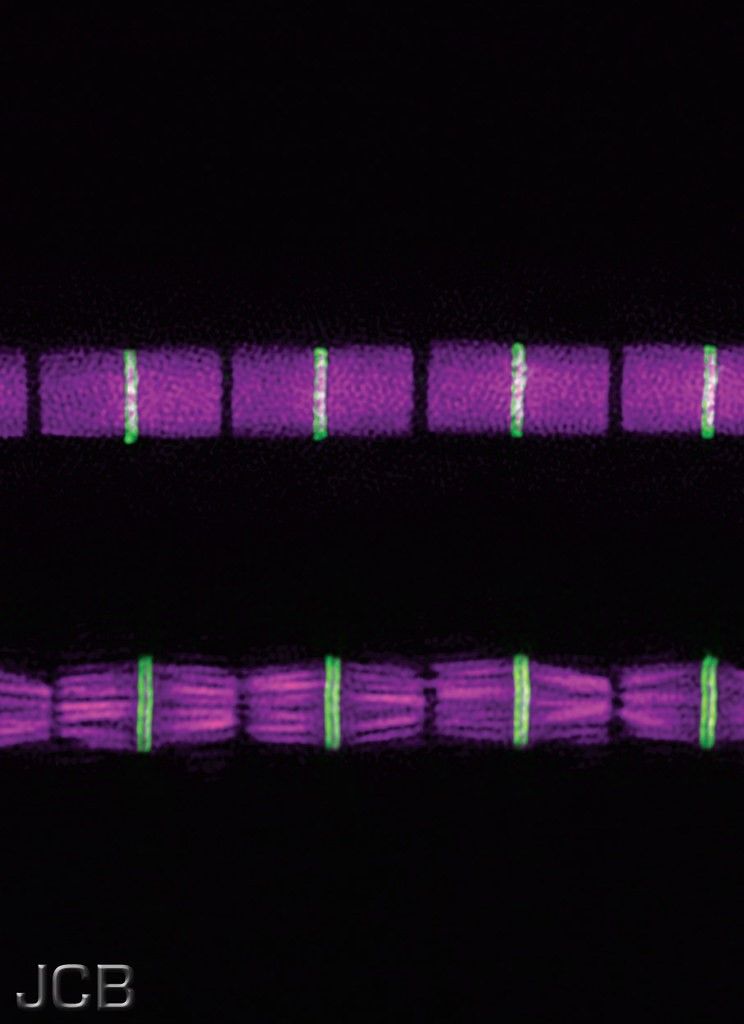
This picture shows the structure of a muscle fibre (or cell), with many sarcomeres lined up. This particular muscle fibre is in contraction, meaning that the actin and myosin filaments are overlapping. The pink portions represent the myosin filaments (A band), meaning the green line is the M line (portion of the myosin filament where there is no actin overlap).
Creative Commons CC-BY-NC-SA 2.0 Source Fernandes and Schöck (2014) J. Cell Biol. 206:559-572
The three types of muscle regenerate in different capacities.
- Smooth muscle is the only type of muscle to retain full mitotic ability, meaning that smooth muscle cells can always divide through mitosis. This is useful for cells like the smooth muscle cells in the uterus, because these need to be able to multiply during pregnancy.
- Skeletal muscle cells cannot divide, meaning that hypertrophy is how skeletal muscle grows. Individual skeletal myocytes can increase their length by adding sarcomeres. Saying this, there is a type of stem cell that exists in skeletal muscle called satellite cells, which can differentiate into skeletal myocytes if the muscle is put under stress.
- Cardiac myocytes cannot regenerate in any significant capacity. This is obviously a bad thing if the myocytes begin to fail, like in heart failure. Instead of regeneration, fibroblasts invade and lay down fibrous scar tissue, which makes the remaining muscle less flexible (which is not good in a heart).
Reviewed by: Dr. Marcus Judge
In this article
There are three types of muscle in the body: skeletal (the muscles used to move the skeleton), cardiac (the muscle in the heart), and smooth (the muscle…
- 16799
