

Next Lesson - Mood Disorders
Core
Anxiety is defined as a feeling of worry, nervousness, or unease about something with an uncertain outcome.
Symptoms of anxiety can include:
- Palpitations
- Sweating
- Trembling or shaking
- Dry mouth
- Difficulty breathing or hyperventilation
- Chest pain or discomfort
- Nausea or abdominal ‘fluttering’
- Feelings of dizziness, light-headedness or faintness.
Feelings of anxiety were essential to survival for human ancestors. However, too much anxiety impairs performance due to distraction, as seen today with for example exam performance - some anxiety is good to help focus the mind, but too much anxiety will hinder rather than help.
This can be shown in the Yerkes-Dodson law seen below:
This image shows the relationship between performance and arousal (or anxiety level).
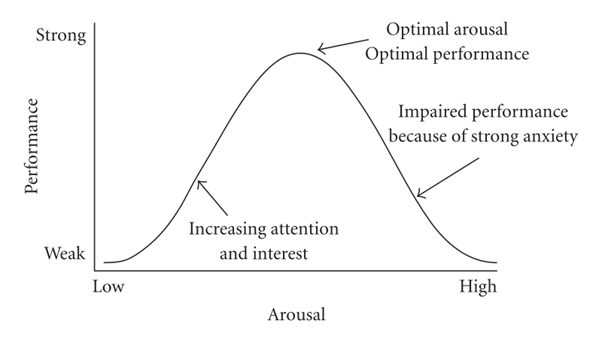
Diagram - The Yerkes-Dodson Law
Licensed under Creative Commons, Source.
While anxiety may feel unhelpful in many situations today, these adaptations offered an evolutionary advantage to ancestors that had to escape life-threatening situations. The body assists this escape through the stress response.
The limbic system is a collection of structures that sit medially in the brain, on the border of the cerebral cortex and the subcortical structures known as the diencephalon. It is responsible for many different systems that help regulate emotions and motivations, especially those related to survival, such as sexual behaviours, hunger, and anxiety. It also contributes to higher cortical functions, such as learning and memory.
Which structures in this region are included in the limbic system is a point of contention, so this is a list of structures most often included:
Amygdala - an almond shaped collection of cells located in the temporal lobe that is particularly involved in anxiety and fear.
Hippocampus - the main function of the hippocampus is with memory, particularly the conversion process of short term memories to long term memories. Bilateral damage to the hippocampi would therefore cause antegrade amnesia, a condition where new long term memories cannot be formed.
Cingulate Gyrus - found superior to the corpus callosum in the medial portion of the brain. This structure is involved in both emotion and memory.
Fornix - a bundle of fibres responsible for transmitting information from the hippocampus to the mammillary bodies, with onward connections to the thalamus.
Hypothalamus - through interactions with the pituitary gland, the hypothalamus can influence many things in the body through the release of hormones into the bloodstream. The hypothalamus also plays a key role in the regulation of the autonomic nervous system.
Thalamus - a large mass of grey matter cells which make up the main relay portion of the brain for both sensory and motor signals.
Other structures that can be considered part of the limbic system but have not been included in this list are: Parahippocampal gyrus, septal nuclei, and mammillary bodies.
This image shows the different structures that make up the limbic system.
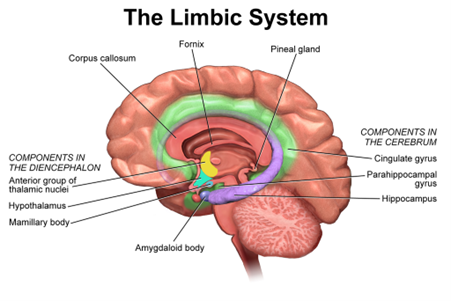
Diagram - The Limbic System
Licensed under Creative Commons, Source.
In a particularly anxiety-inducing situation, the limbic system and the cortex work together to prompt the hypothalamus, which in turn activates the motor system, increasing blood supply to muscles, and the sympathetic nervous system, activating the ‘fight or flight’ response.
This diagram shows the process of prompting the motor system and the sympathetic nervous system in response to anxiety.
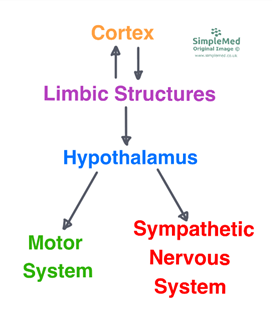
Diagram - The Stress Response
SimpleMed original by Dr. Maddie Swannack
The stress response can be split into three phases:
Alarm
The initial prompting of fear in a human will cause activation of the sympathetic nervous system, releasing noradrenaline and causing the release of adrenaline from the adrenal medulla and cortisol (known as the stress hormone) from the adrenal cortex. This gives the initial burst to run away or fight the stressor.
Resistance
Adrenaline has a half-life of 2-3 minutes, meaning the high levels of adrenaline in the blood from the alarm response do not last long. Cortisol has a much longer half-life, allowing the maintenance of the stress response if needed.
Exhaustion
Prolonged stressful situations result in continued cortisol release. Over time, this leads to muscle wasting, suppression of the immune system and hyperglycaemia.
The stress response can therefore become a problem if the stress is not something that is quickly escapable, like stress in the modern world.
The main neurotransmitters that influence anxiety disorders are serotonin and GABA.
GABA is the main inhibitory neurotransmitter in the brain, and decreased levels of GABA are seen in the brains of patients diagnosed with anxiety disorders. Benzodiazepines increase GABA transmission in the brain, so can help reduce anxiety.
Serotonin receptors exist on the hippocampus, so increasing serotonin in the limbic system through Selective Serotonin Reuptake Inhibitors (SSRIs) can lead to a reduction of anxiety.
Anxiety disorders are a collection of psychiatric disorders where the predominating feature is a feeling of anxiety. There are many different types.
Physical Conditions that Present Similarly to Anxiety Disorders
A number of medical conditions can present similarly to anxiety disorders and should be investigated for when presented with treatment-resistant anxiety. Examples include:
- Hyperthyroidism
- Hypoglycaemia
- Anaemia
- Cushing’s Disease
- Intoxication with or withdrawal from alcohol
- Excess caffeine intake
Risk Factors for Anxiety Disorders
Anxiety disorders have a number of risk factors, that can be classified into predisposing, precipitating and perpetuating factors:
Predisposing
Predisposing factors are factors that the patient cannot change and that accumulate to increase the likelihood of anxiety. They include:
- Genetics
- Childhood upbringing, especially parental demands for high achievement
- Living alone
Precipitating
Precipitating factors are factors that exist in the patient’s life that, combined with predisposing factors, encourage the presentation of anxiety at that point. Examples include:
- Chronic illness
- Relationship problems
- Unemployment
Perpetuating
Perpetuating factors are factors that encourage the persistence of anxiety disorders once they are already established. They are often seen as barriers to successful treatment. Examples include:
- Chronic illness
- Living alone
- Negative thinking that perpetuates anxiety - for example, specific worries about other noticing the patient’s anxiety.
Generalised Anxiety Disorder (GAD)
GAD is a condition characterised by symptoms of anxiety present most days for a period of months that is causing some impairment of function. The anxiety may be generalised (‘free floating’) or specific (for example related to family, finances, school / work), and may be associated with other physical symptoms such as muscle tension, restlessness, sweating, irritability, or sleep disturbance.
GAD is estimated to affect 4 in 100 adults in the UK (source).
GAD is treated in the UK with psychological therapy first line, such as cognitive behavioural therapy (CBT), with pharmacological therapy such as SSRIs considered if symptoms are significant or persistent. Benzodiazepines are not recommended for routine treatment and are reserved for short term use in acute crises.
Panic disorder is a condition characterised by a history of repeated attacks of intense subjective fear that come on rapidly, resulting in a pervasive anxiety about further attacks occurring.
It is acutely difficult to assess, as the patient is not often having a panic attack at presentation to the GP, but a diagnosis can be made on history alone. Panic disorder can be associated with agoraphobia, which is the avoidance of exposed situations to try to avoid the onset of panic.
It is especially important with panic disorders to rule out physical causes of the symptoms of a panic attack: hyperthyroidism, hypoglycaemia, myocardial infarction, focal epilepsy, withdrawal from substances, and vestibular disorders such as Meniere’s Disease can all present with discrete episodes of symptoms characteristic of a panic attack.
Treatment of panic disorder is initially with education for the patient and family, alongside cognitive behavioural therapy. Pharmacological therapy can be trialled second line, especially if the disorder is causing drastic problems with function day to day.
Social phobias are specific fear of being around other people and having to interact with them, often associated by the fear of being watched and criticised. Many people experience some degree of social anxiety, such as mild nervousness before playing in a concert or speaking to a crowd. Social phobias are therefore considered to be an exaggerated version of normal social anxiety, where the patient’s condition prevents them from entering situations where they will have to interact with others.
Again, this can be a difficult condition to diagnose as patients suffering with social phobias are less likely to present to their GP to talk about their condition. Management of this condition is initially through psychological interventions like CBT, with consideration of pharmacological interventions later. There is also some evidence that exposure therapy can help, but that the condition will often improve over time. (source)
A phobia is an overwhelming and debilitating fear relating to a very specific object, place, situation, feeling or animal. The symptoms of anxiety occur only when in proximity to the source of the phobia, or in severe cases, they may occur only if thinking about the source.
Most phobias can be overcome with gentle exposure therapy as part of a self-help program. More intensive therapies, such as CBT, being employed only if the phobia is causing severe effects in day to day life.
Obsessive compulsive disorder (OCD)
Obsessive compulsive disorder is a psychiatric disorder that is present for at least two weeks, and it is made up of two parts:
- Obsessions are unwanted, intrusive thoughts, images or urges that repeatedly enter the person’s mind. They cause the patient distress. An example of a compulsion may be intrusive images where the patient sees themselves stabbing someone.
- Compulsions are repetitive behaviours that the patient feels driven to perform to reduce the power that the obsessions appear to have. An example of a compulsion relating to the obsession above may be having to leave and re-enter the kitchen 7 times before touching a knife.
The management of OCD depends on the severity of the effect that the condition has on the patient day to day. Initially, psychological therapy is preferred. A particular type of therapy called exposure and response prevention (ERP) is used to help patients go through their obsessional thoughts without completing the corresponding compulsion. Pharmacological treatment is often used alongside psychological therapy in moderate to severe OCD, as the condition can significantly impact the patient day to day.
Post-Traumatic Stress Disorder (PTSD)
Post-traumatic stress disorder may develop after exposure to intensely terrifying or threatening events. It is characterised by the following, lasting more than one month:
- Re-experiencing - vivid, intrusive memories, flashbacks or nightmares that often involve more than one sensory modality and are associated with strong emotions.
- Avoidance - both of actively thinking about the event, and avoidance of situations that might accidentally prompt remembrance.
- Hypervigilance - enhanced startle reactions and persistently mistaking benign things as a threat.
PTSD vs Acute Stress Reaction
Acute stress reaction refers to the initial traumatic symptoms that originate immediately after the traumatic event. PTSD refers to the long-term symptoms due to the trauma.
PTSD can occur with or without an initial acute stress reaction, and not every acute stress reaction progresses into PTSD.
Acute stress reactions come on very quickly after trauma, and last less than one month. They are usually characterised by dissociative symptoms.
PTSD usually comes on more slowly, and must last more than one month. Symptoms include re-experiencing, avoidance and hypervigilance.
Risk Factors
Examples of events that are associated with PTSD include war, serious accidents, sexual assault, trauma related to health experiences such as childbirth or intensive care admission. Therefore, exposure to these events increases the risk of PTSD.
Other risk factors for PTSD include:
- First responders - by definition, first responders are more likely to be exposed to traumatic events.
- Previous psychiatric disorders increase the risk of PTSD.
- Approximately 2 in 100 women have PTSD postnatally. (source)
- Military personnel have additional risk factors:
- Increased duration of combat exposure
- Poor social support, and unmarried status
Management
The first step to managing PTSD is providing information and support, including information on peer support groups if the patient feels they may help.
A specific type of therapy called Eye Movement Desensitisation and Reprocessing (EMDR) has been developed for PTSD, and other psychological therapies can also be used. Pharmacological treatments such as antidepressants may be helpful; antipsychotics are not first-line and are usually reserved for specific indications.
Edited by: Dr. Marcus Judge
Reviewed by: Adrian Judge
In this article
Anxiety is a feeling of worry, nervousness, or unease. It was a useful adaptation for our ancestors who needed anxiety to prep the body for the ‘fight or…
- 664

{kind=link}
{kind=link}