

Next Lesson - Movement Disorders
Core
The reticular formation is a set of grey matter nuclei that are spread throughout the brainstem that are functionally linked (see below). The primary function of this is to keep the cerebral cortex ‘awake’ by maintaining behavioural arousal (not to be confused with sexual arousal) and consciousness.
Arousal is the state of being awake and is important to cause goal-seeking behaviour (such as looking for food, maintaining mobility and the fight or flight response).
Consciousness is the awareness of both the internal and external environments. The preservation of this requires the reticular formation and cortex to be functioning normally and appropriately connected to each other. Consciousness is a generally very slippery concept to grasp and understand fully, so it’s completely reasonable if you find it difficult to understand.
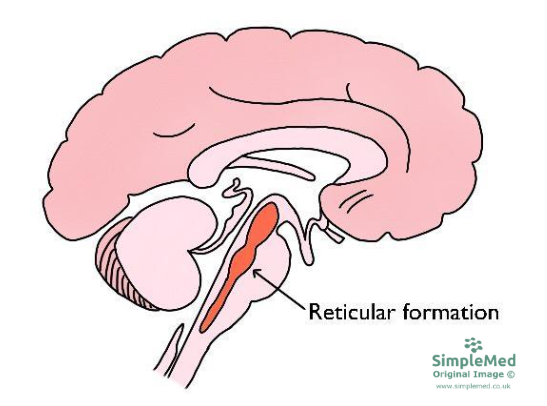
Diagram - The Reticular Formation found throughout the Brainstem
SimpleMed original by Dr. Keertana Anne
These functions are carried out by the activation of the ascending reticular activating system (ARAS), which is the pathway connecting the reticular formation to the cerebral cortex. This connection forms a positive feedback loop, meaning the output produced is always binary (either asleep or awake, for example).
The reticular formation functions on a system of inputs and outputs. It receives inputs from the sensory systems and the cortex itself, and sends outputs to the thalamus, hypothalamus and basal forebrain nuclei (and also to the spinal cord, which is responsible for maintaining muscle tone). The reticular formation sends these outputs via three major relay nuclei, and these then project onto the cortex (see below).

Diagram - The Reticular Activating System
SimpleMed original by Dr. Keertana Anne
The use of cholinergic and histaminergic fibres in the maintenance of the ‘awake’ state explains the action of drugs such as anticholinergics and antihistamines, and why they produce a sedative or drowsy effect on the person.
Massive lesions of the ARAS itself, or the connection between the ARAS and the cerebral cortex, can cause a variety of disorders of consciousness. These are explored later on in this article.
Clinical Assessment of Consciousness
There are three primary ways of assessing the conscious state of the brain, and each of them are used in different situations.
Note: ACVPU is a commonly used UK modification of the AVPU scale that includes assessment of new confusion.
The AVPU scale is used in emergency situations to assess a patient’s response to a variety of stimuli. It is a simple tool used in clinical settings like wards to quantify a patient’s conscious level, and on observation charts in the UK, a score of anything other than A for Alert prompts review by the medical team.
Alert - the patient is fully awake and shows no evidence of confusion. They will be able to spontaneously open their eyes, speak or move their body.
Confused - the patient is able to respond to you in some way, but is not orientated to place, person or time. This is a new change for the patient, and therefore indicates a potential deterioration in consciousness level.
Responsive to voice - the patient will respond in one of three ways when prompted by a voice. This could be opening the eyes; a verbal response such as a groan; or a slight movement of the limbs.
Responsive to pain - the patient will be able to respond in one of three ways when a painful stimulus is applied. Examples of this include squeezing the fingers or a trapezius squeeze. Central painful stimuli should be applied carefully to avoid injury.
Unresponsive - the patient is not responsive to any of the above stimuli.
The Glasgow Coma Scale is also used to assess the conscious level of a patient in emergency situations and for subsequent assessment in hospital. See the table (Figure 3) for the breakdown of the scoring.
Eye Opening
4 Spontaneous eye opening Normal cortical and brainstem function.
3 Response to speech Reduced cortical function, preserved brainstem function
2 Response to pain Impaired cortical function, preserved brainstem function
1 No response Severe damage to brainstem and cortex
Verbal Response
5 Orientated in time / place Normal cortical and brainstem function
4 Confused speech Reduced cortical function, preserved language centres
3 Inappropriate words Damage to language centres likely
2 Incomprehensible sounds Cortical damage with brainstem mediated groans
1 No response Severe damage to brainstem and cortex
Motor Response
6 Obeys commands Normal functions of cortex, spinal cord, and auditory system
5 Localised to stimuli Lost higher cortical functions, preserved motor and sensory
4 Withdraws from pain Physiological reflexes preserved, limited cortical function
3 Flexor response to pain Suggests a lesion above the midbrain
2 Extensor response to pain Suggests a lesion below the midbrain - abnormal response
1 No response Severe damage to brainstem and cortex
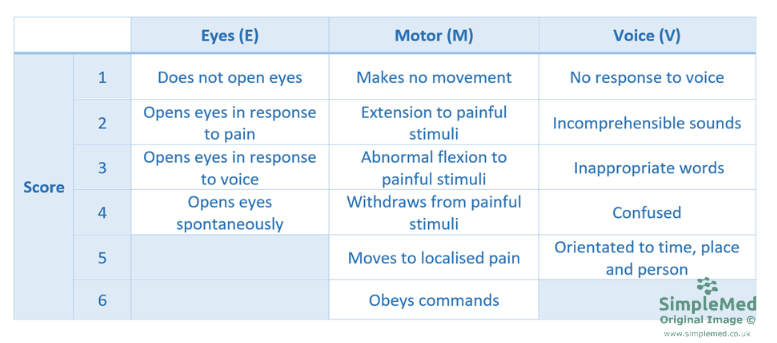
Diagram - The Glasgow Coma Scale
SimpleMed original by Dr. Keertana Anne
Patients are given an overall score and also a breakdown of the individual components, for example GCS 11 = E3 M4 V4. A score of 15 is the highest possible, and 3 is the lowest (because for each category, no response results in a score of 1). The Glasgow Coma Scale is only used in living patients and does not apply to brain death.
So a GCS of 15/15 indicates that the brainstem, spinal cord, cerebral cortex and auditory processes are all functioning normally. A GCS of lower than this indicates that there is some problem in one of those places: for example, a patient with reduced consciousness levels due to drugs or alcohol would struggle to process and carry out instructions but would still demonstrate motor responses to painful stimuli.
The Electroencephalogram (EEG)
The EEG is a test used to measure the electrical activity in the brain. It works by placing electrodes a few centimetres apart on the scalp, and these measure the activity of thousands of neurones in a specific region of the cortex. The EEG has a high temporal resolution (meaning it is good at measuring short periods of time - milliseconds), but a low spatial resolution (meaning that it is bad at visualising the impulses in 3D, owing to the distance between each sensor on the scalp - see below).
Diagram - An EEG Recording Cap
Licensed under Creative Commons, Source.
This piece of equipment is used to detect neuronal synchrony. This occurs when the neurones in the brain are deprived of sensory input, both physiologically (sleep) and pathologically (epilepsy) and begin to fire more regularly. EEG patterns can also be affected by changes in conscious states such as a coma or brain death.
Sleep is a physiological, recurring process that the human body undergoes and is considered a partially unconscious state of the mind. During the process, the mind and body are both unable to react to stimuli in a way they would normally do if awake, however the brain itself remains very active. The functions of sleep are mostly unknown, but some theories are that sleep has a role in memory consolidation, clearance of extracellular debris, and ‘resetting’ of the CNS.
It can be classified into two categories - Rapid Eye Movement (REM) and non-Rapid Eye Movement (non-REM) and the body cycles through these two stages while asleep (see below).
During REM sleep, the EEG pattern is similar to that of an awake person, and the sleeper is able to dream. The body has decreased muscle tone during this time due to the inhibition of lower motor neurons, however some functions are preserved (such as penile erection), despite widespread skeletal muscle atonia.
Non-REM sleep is very complex and is traditionally described as four stages, with stage 4 being the deepest sleep. In modern classifications, these are grouped into three stages (N1 to N3). Unlike in REM sleep, the muscles are not paralysed (hence a person may be able to sleepwalk by being stuck in a non-REM stage of sleep) and people do not dream. It occurs due to the deactivation of the ARAS that normally ensures a person remains in an awake state.
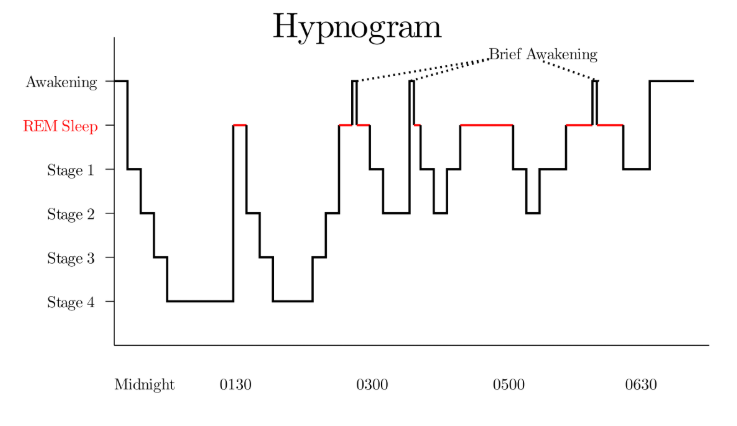
Diagram - Hypnogram showing the Fluidity between the Different Stages of Sleep
Licensed under Creative Commons, Source.
In studies conducted, sleepers were seen to normally go through about 6 cycles of sleep per night (made up of REM and the 4 stages of non-REM). The EEG below depicts the stages of being asleep and awake, and the information below it describes characteristic features of each. Notice how as the person falls into a deeper sleep (Stage 4), the neurones become more regular in their firing - as mentioned earlier in the article this is called neuronal synchrony.
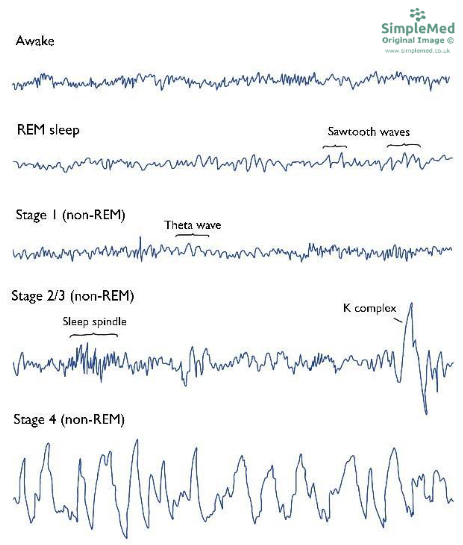
Diagram - An EEG depicting the Different Stages of Sleep
SimpleMed original by Dr. Keertana Anne
Awake - characterised by beta waves, typically in the range of around 13 to 30 Hz.
Stage 1 Sleep - background of alpha waves, with interspersed theta waves, frequency of approximately 5 Hz.
Stages 2 / 3 Sleep - background of theta waves, with interspersed sleep spindles (high frequency bursts from the thalamus) and K-complexes (which represent the ‘intrinsic’ pattern of brainwaves in the cortex).
Stage 4 Sleep - regular delta waves predominate at a frequency of around 1 Hz. These are similar to the K-complexes seen earlier.
REM Sleep - beta waves predominate, as the patient is dreaming, and this is equivalent to being awake.
Insomnia - a condition involving difficulty getting to sleep or staying asleep. It is commonly due to an underlying psychiatric condition such as anxiety disorders.
Narcolepsy - a rare condition presenting with difficulty regulating sleep-wake cycles, resulting in a person being overcome by sleep at inappropriate times. Many narcoleptics also suffer from cataplexy, a sudden loss of muscle strength.
Sleep Apnoea - a common condition often caused by excess neck fat leading to compression of airways during sleep, and frequent waking. It causes excessive daytime sleepiness and is treated with weight loss and CPAP machines which introduce pressure to the airways to encourage the airways to remain open.
Disorders of consciousness are medical conditions caused by damage to the areas of the brain that regulate consciousness (e.g. the reticular formation).
Brain injuries can be categorised into three mechanisms of injury:
- Traumatic, for example as a result of a car accident
- Non-traumatic, caused by acute health conditions such as a stroke or infections
- Progressive brain damages caused by conditions that gradually worsen over time, such as in Alzheimer’s disease or brain tumours).
These disorders can range from less severe to life threatening depending on the extent of damage done. Here are a few examples, ranging from least to most severe:
Locked-in syndrome: This is caused by the occlusion of the basilar or pontine arteries, resulting in the loss of nervous system function below the level of occlusion, usually leaving the patients with motor control only of the oculomotor nerve. The patient is aware of the external environment but is unable to respond to any stimuli, except through eye movements and blinking. They also go through similar sleep-wake cycles as a healthy person.
Minimally conscious state: In this state, patients are less aware of their surroundings in comparison to locked-in syndrome but still have brief periods of consciousness. During this time, they are able to follow basic commands and perform purposeful behaviour.
Persistent vegetative state: This is caused by widespread cortical damage. Patients have a detectable sleep-wake cycle in this state but are fully unaware of their surroundings. They are only able to display reflexive and non-purposeful behaviour and are sometimes able to open their eyes spontaneously.
Coma: Similar to persistent vegetative state, patients have widespread cortical damage and also have brainstem damage on top of it. They lack awareness of their surroundings and do not respond to any stimuli. Unlike vegetative states, the patient does not have a discernible sleep-wake cycle. Comas can be medically induced following brain injury using sedative or anaesthetic drugs.
Brain death: This involves irreversible loss of brainstem function, with or without widespread cortical damage, and is a legally defined state. Diagnosis is based on strict clinical criteria rather than EEG findings.
Edited by: Dr. Maddie Swannack
Reviewed by: Adrian Judge
In this article
The reticular formation is a group of nuclei that is distributed throughout the brainstem, and acts to keep the cerebral cortex awake.
- 687

{kind=link}
{kind=link}