

Next Lesson - The Cerebellum: Circuits, Coordination and Clinical Signs
Core
In the somatic (voluntary) motor system of the body, the neural pathways are made up of two neurones in a chain.
The first is called the upper motor neurone, and they exist completely within the central nervous system; their cell body is located in the primary motor cortex, which is in the precentral gyrus of the frontal lobe.
The second neurone in the chain is called the lower motor neurone, and these cross from their cell body located in the central nervous system (specifically in the brainstem or the ventral horn of the spinal cord), to their synapse with skeletal muscle in the peripheral nervous system.
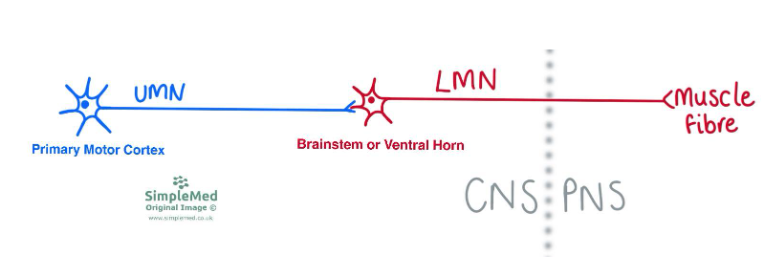
Diagram - The Relationship of Upper Motor Neurones and Lower Motor Neurones
SimpleMed original by Dr. Maddie Swannack
Lower motor neurones are the neurones that connect the central nervous system to the muscles - they are spinal or cranial nerves. They are controlled by upper motor neurones, which descend through the cord or brainstem and synapse on LMNs.
Their cell bodies are found in the ventral horn of the spinal cord, and in cranial nerve motor nuclei (oculomotor nucleus, trochlear nucleus, trigeminal nucleus etc). The locations that the cell bodies of LMN can be found are shown in colour on the image below. Some of the cranial nerve nuclei have eponymous names, but for general understanding it is fine to know them by the cranial nerves they supply.
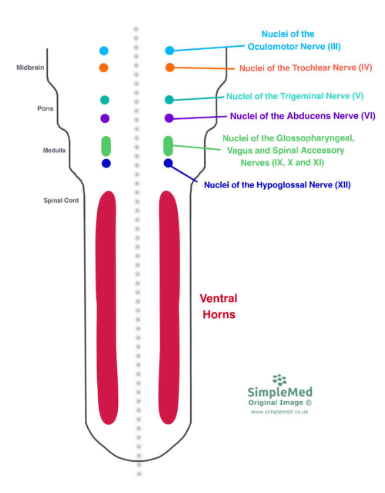
Diagram - The Different Potential Sites for Cell Bodies of Lower Motor Neurones
SimpleMed original by Dr. Maddie Swannack
Lower motor neurones participate in spinal reflexes without the involvement of upper motor neurones.
When considering the patellar reflex as a monosynaptic reflex arc, the patellar tendon is struck with a hammer, this is detected by the stretch of the muscle spindle fibres, and the quadriceps contract, straightening the leg. This is shown in the image below, with the sensory neurone shown in red and the LMN shown in green.
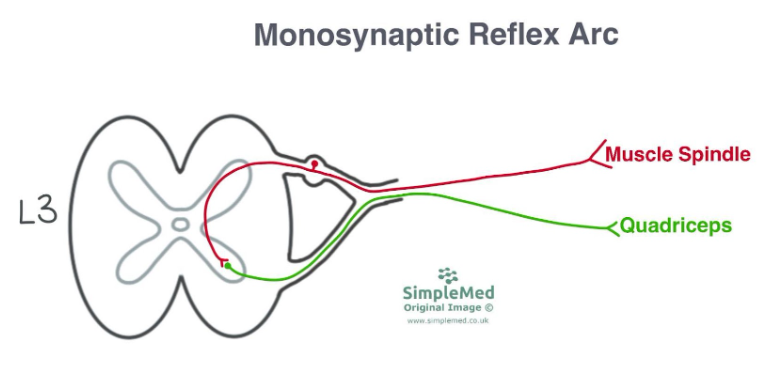
Diagram - The Monosynaptic Reflex Arc of the Patellar Reflex (L3-L4)
SimpleMed original by Dr. Maddie Swannack
However, in reality, although the quadriceps contraction is mediated by a monosynaptic connection, effective knee extension also requires inhibition of the hamstrings. This occurs via a parallel polysynaptic pathway involving an inhibitory interneurone, a process known as reciprocal inhibition. The diagram below shows how the sensory neurone detecting the tendon hammer sends impulses to both the quadriceps and the hamstrings via lower motor neurones, but that the impulse to the hamstrings goes via an inhibitory interneurone, causing contraction of the quadriceps muscles and relaxation of the hamstrings.
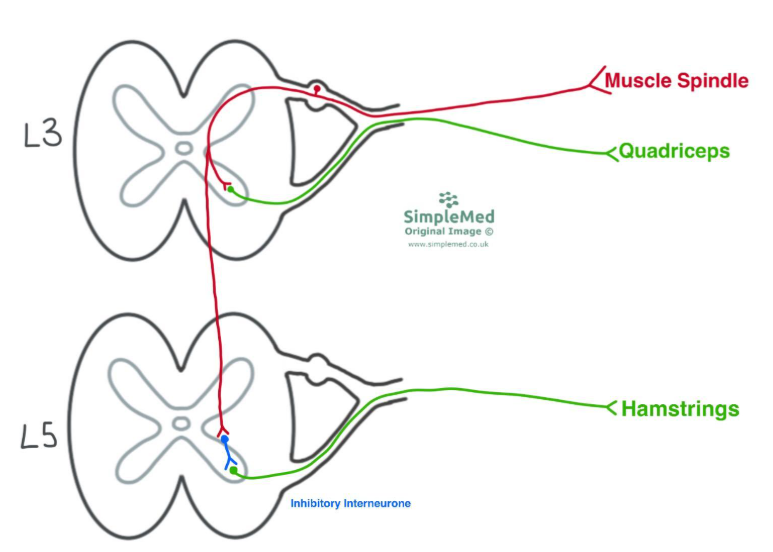
Diagram - The Polysynaptic Reflex Arc of the Patellar Reflex at L3 and L5
SimpleMed original by Dr. Maddie Swannack
Lower motor neurones can be damaged anywhere along their path from the cell body (within the CNS), along the axon to the neuromuscular junction. The most common site for lower motor neurone injury is the axon, which is also known as a peripheral nerve injury.
The following signs can be seen in the muscles supplied by the damaged lower motor neurones:
- Weakness (due to denervation)
- Areflexia (due to denervation)
- Wasting (due to loss of nutritional support to the muscle from the LMN)
- Hypotonia (due to loss of the background action potentials and very small contractions within the muscle that result in tone)
- Fasciculation (due to up-regulation of nicotinic acetylcholine receptors (nAChRs) in the muscle to try to compensate for denervation)
Upper motor neurones are found in the primary motor cortex (precentral gyrus). They synapse onto LMNs directly (or indirectly) in the ventral horn or cranial nerve motor nuclei.
The net effect of UMNs on LMNs is inhibition - this explains most of the features of UMN lesions
Their axons descend from the motor cortex through the following structures:
- Corona radiata of the pre-central gyrus
- Internal capsule
- Cerebral peduncle in the midbrain
- Pons
- Medullary pyramids
- Decussation of the pyramids (in the caudal medulla)
- Lateral corticospinal tract (in the lateral funiculus of the cord)
- Ventral horn of the spinal cord
- Synapse (usually indirectly via inhibitory interneurones) on LMNs in the ventral horn of the spinal cord.
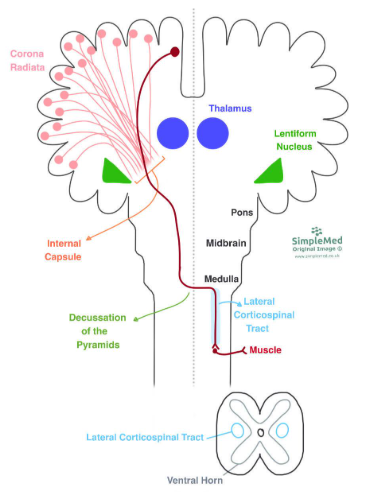
Diagram - The Path of an Upper Motor Neurone from the Pre-Central Gyrus to the Synapse of the Lower Motor Neurone
SimpleMed original by Dr. Maddie Swannack
The lateral corticospinal tract is involved with fine motor control in the limbs.
The upper motor neurone cell bodies exist in the grey matter of the precentral gyrus. They are organised according to the homunculus, with the cell bodies of neurones controlling the legs medially and the cell bodies of neurones controlling the hands laterally.
The axons of all the upper motor neurones converge down the same path, called the Corona Radiata. This is a bundle of axons that forms the white matter structure of the internal capsule as it runs between the thalamus and the lentiform nucleus. The internal capsules run at an oblique (diagonal) angle from the hemispheres of the brain to the midbrain of the brainstem.
Here, there are two different paths for UMN depending on which type of muscles they supply. The majority of UMN are those supplying distal muscles that need fine control, like the muscles of the fingers, and these travel through the lateral corticospinal tract. The remaining are muscles that need endurance, like the paraspinal muscles, and these travel in the anterior corticospinal tract. At this level of neuroanatomy, you don’t need to know much at all about the anterior corticospinal tract; it is included here just for increased understanding.
Distal Muscles - Lateral Corticospinal Tract
From the internal capsule, the axons of the upper motor neurones enter the brainstem through the cerebral peduncles of the midbrain. The axons descend through the midbrain, the pons and most of the medulla. In the caudal region (inferior region) of the medulla, the axons of the upper motor neurones decussate (cross the midline) to form the lateral corticospinal tract and descend on the contralateral side of the spinal cord.
The UMN synapses with the LMN at the level that the LMN will exit the CNS.
Most of the neurones that project onto lower motor neurones are inhibitory in nature.
This is very important clinically because the natural state of a muscle controlled by a lower motor neurone is in contraction - this means that these inhibitory connections allow for muscle relaxation. If these connecting neurones were not inhibitory in nature, it would be very difficult to relax any muscles.
This idea can be summarised by the idea that there is net inhibition of LMNs by UMNs via inhibitory interneurons. This means that most of the features of upper motor neurone lesions result from the loss of the inhibition of lower motor neurones, and are therefore signs of over-activation of lower motor neurones.
The upper motor neurones that supply the muscles of the face originate in the precentral gyrus, as with all upper motor neurones. However, these UMN do not decussate in the medulla and synapse in the spinal cord as this would be too far inferior to supply the muscles of the face.
They in fact descend through the internal capsule and enter the corticobulbar tract, where they synapse with the facial nerve nucleus in the pons. The pattern of decussation applies to the upper motor neurone inputs rather than the lower motor neurone axons.
The facial motor nucleus is a special case of a cranial nerve motor nucleus, in that it is split into two halves - the top half of the nucleus contains the cell bodies of LMN that supply the muscles of the upper face, and the bottom half of the nucleus contains the cell bodies that supply the lower half of the face.
The UMN supply for the inferior portion of the facial nerve nucleus (supplying the lower half of the face) is contralateral.
The UMN supply for the superior portion of the facial nerve nucleus (supplying the upper half of the face) is bilateral, meaning it has inputs from both sides of the brain.
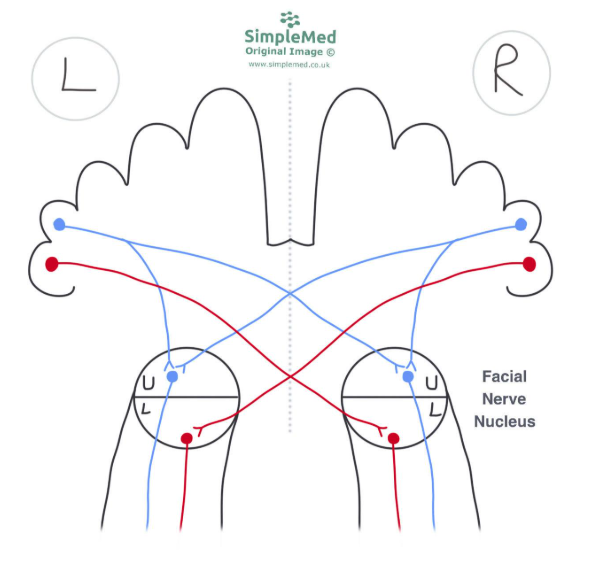
Diagram - The Nature of Inputs to the Facial Nerve Nuclei
SimpleMed original by Dr. Maddie Swannack
This knowledge can be used to distinguish between a facial nerve lesion (LMN) and a brain injury (UMN).
A lesion of the facial nerve itself causes paralysis of one entire side of the face, because the innervation to the upper and lower half of the face are damaged after the nucleus. This is called Bell's palsy, and the side of the loss indicates the side of the lesion, because the LMN will innervate the muscles on the side of the injury.
With an upper motor neurone lesion, for example with a stroke, there is loss of UMN input to the lower face on the affected side. However, because the top half of the face receives impulses from both hemispheres of the brain, the upper half of the face still receives sufficient undamaged input. This creates a ‘forehead sparing’ pattern. With an UMN lesion, the side of the weakness is contralateral to the side of the lesion. For a visual demonstration of this, see the image below.
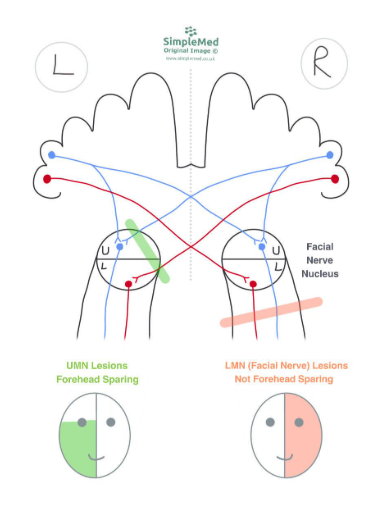
Diagram - Motor Neurone Lesions
SimpleMed original by Dr. Maddie Swannack
When UMNs are damaged, there is loss of stimulation (and therefore the loss of the inhibition) of the lower motor neurones. This means that the signs of upper motor neurone lesions are:
- Weakness (due to loss of direct excitatory inputs onto LMNs from UMNs)
- Hypertonia (due to loss of descending inhibition - remember that the net effect of UMNs on LMNs is inhibition)
- Hyperreflexia (same origin as hypertonia - an overactive reflex arc)
- Extensor plantar reflexes (see below)
Babies have a different set of reflexes than adults do due to their upper motor neurones being immature, and therefore not having yet developed that inhibition on the lower motor neurones.
One example of this is the plantar reflex, which is characterised by the direction of movement of the toes when the sole of the foot is stimulated. The normal, adult response is for the toes to flex down, almost as if they are trying to protect the sole of the foot. In babies, and in those with upper motor neurone lesions, the response is to extend the toes back. With age, usually around when the child starts walking, the immature, upgoing response turns into the mature, downgoing response. This means that testing the direction of the plantar reflexes is a good way of checking for upper motor neurone lesions.
When a baby experiences a sudden loss of support, their arms will splay out to the sides as if to catch themselves. This is another example of an upper motor neurone reflex that occurs in babies and that is lost as the baby ages and the inhibition provided by upper motor neurones matures. It is a primitive, protective reflex that is lost with age as the child can move themselves out of danger more easily.
The third example of an upper motor neurone reflex that occurs in babies is the palmar grasp. This is a reflex designed to help tiny babies hold onto their caregivers, and their hands close around anything that touches the palm. It is often seen with small babies grabbing the hair or clothing of their caregivers. It is a primitive reflex designed to keep babies safe, and again disappears as the baby ages and as the upper motor neurone inhibitory pathways mature.
Spinal shock is a phenomenon that occurs immediately after an acute UMN lesion and can last days to weeks. Initially there is flaccid paralysis with areflexia (as in LMN lesions), but tone then increases (becoming hypertonia) and reflexes become exaggerated (hyperreflexia). The mechanism of this is unclear, but is related to neuroplasticity in the spinal cord.
Edited by: Dr. Marcus Judge
Reviewed by: Adrian Judge
In this article
The motor system is made up of two neurones, the upper motor neurone in the central nervous system and the lower motor neurone, which have their cell…
- 642
