

Next Lesson - Raised Intracranial Pressure
Core
A stroke is a serious, life-threatening medical condition that occurs when the blood supply to a portion of the brain is cut off. It is also known as a cerebrovascular accident.
When the blood supply is cut off, the supply of oxygen and glucose to the brain is cut off. This prevents the production of ATP in this portion of the brain, because respiration needs oxygen and glucose to occur. With limited amounts of ATP, the membrane potentials needed for neuronal transmission stop, and so no neuronal transmission occurs.
Given that a stroke is a loss of the blood supply to one portion of the brain, there are two main types of stroke:
Ischaemic strokes are the most common type of stroke, making up around 85% of strokes (source). The arterial supply to a portion of the brain is cut off by a clot in the vessel. Most often, this clot has formed somewhere else in the body and travelled via the arterial system to the brain, called a thromboembolism.
Haemorrhagic strokes make up around 15% of strokes. This occurs when a vessel in the skull breaks open, causing a bleed in the brain; this can either prevent the blood getting to the area supplied by the end of the artery, or cause an increase in pressure within the skull which compresses the artery and prevents blood flow.
There are some causes of stroke that do not fit neatly into the ischaemic or haemorrhagic categories. This includes conditions such as carotid artery dissection, where blood flow to the brain is reduced without a typical intravascular clot or intracerebral haemorrhage.
A transient ischaemic attack (or TIA) is often described as a mini-stroke, where stroke-like symptoms come on and then resolve, usually within 1 hour. It is now defined by the absence of acute brain infarction on imaging, rather than by a fixed time limit.
There are a number of risk factors for ischaemic strokes, which are very similar to risk factors for other vascular pathologies such as angina, heart attacks and peripheral vascular disease. (source)
Like with any condition, the risk factors can be split into modifiable and non-modifiable factors.
Modifiable risk factors include:
- Smoking
- High Cholesterol
- Diabetes
- High blood pressure
- Obesity
- Excessive alcohol intake
- Unmanaged atrial fibrillation
Non-modifiable risk factors include:
- Increased age
- Family History of stroke or TIA
- Ethnicity - South Asian, African or Caribbean ethnicities carry higher risk
- Personal History of stroke or TIA
- Other medical conditions that make the blood more coagulopathic (likely to clot) such as cancer.
The main risk factor for haemorrhagic strokes is hypertension, a modifiable risk factor.
The risk is also increased by use of anti-coagulant medication, which increases the risk of all bleeding.
What to do if we suspect a stroke?
An acute stroke in a patient presenting to the emergency department is something that requires quick action. This is because the treatments for different types of stroke (ischaemic or haemorrhagic) are very different, and the success in restoring functions that have been lost is time-dependent. This means that in a patient presenting with symptoms that may be consistent with an acute stroke, urgent assessment and rapid CT head imaging are crucial.
The purpose of the CT head is to rule out a haemorrhagic stroke. In the early stages of an ischaemic stroke, CT may appear normal, although subtle early ischaemic changes can sometimes be seen before established tissue death. If there are no signs of haemorrhage on head CT, the stroke is deemed to be likely ischaemic in nature and the treatment for that can be started.
An MRI head would show any areas of ischaemia, making it more definitive in diagnosis of ischaemic stroke. However, MRIs take longer than CTs, and are often not as easily available, making CT scan the initial imaging mechanism of choice.
The blood supply to the brain comes from two main sources, the internal carotid artery and the vertebral arteries, which come together to form the Circle of Willis. The Circle of Willis has three main terminal branches (the anterior cerebral artery, the middle cerebral artery, and the posterior cerebral artery), which create three main arterial territories. The blood supply to the brain is also divided into the anterior and posterior circulations, an artificial divide through the posterior communicating artery, as shown on the diagram below.
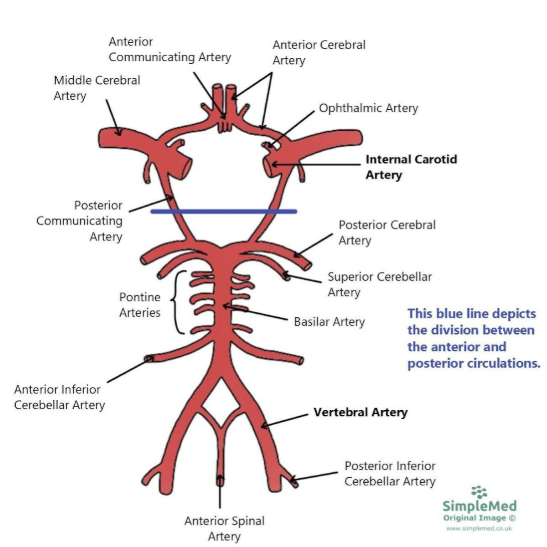
Diagram - The Blood Supply to the Brain
SimpleMed original by Dr. Keertana Anne
For more information on the Arterial Supply of the Brain, please see our third article in this series here.
Territories of Cerebral Arteries
There are three terminal branches of the Circle of Willis. These are the anterior cerebral artery (ACA), the middle cerebral artery (MCA) and the posterior cerebral artery (PCA).
Each of these arteries supplies a different portion of the brain, meaning that a blockage in supply of one of them will result in symptoms that can be localised to a specific region. This means that the likely location of an infarction can be worked out due to the symptoms.
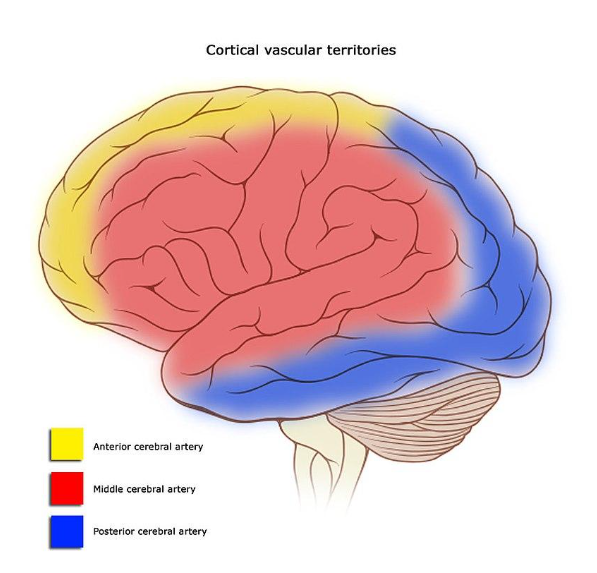
Diagram - The Territories Supplied by the Three Terminal Branches of the Circle of Willis on the Lateral Side of the Brain
Licensed under Creative Commons, Source.
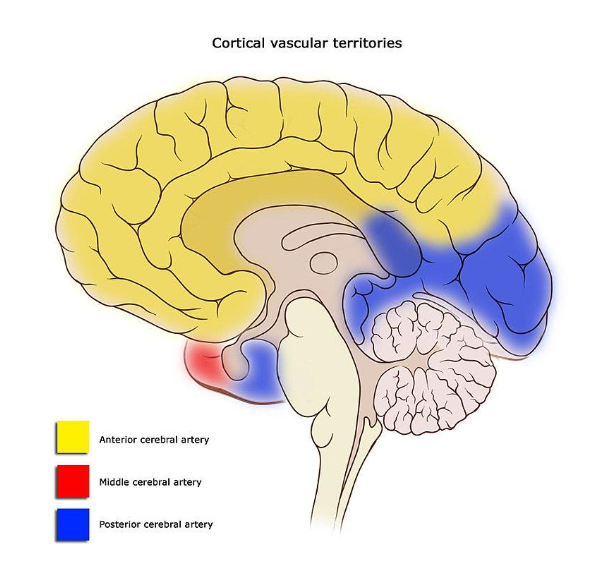
Diagram - The Territories Supplied by the Three Terminal Branches of the Circle of Willis on the Midline of the Brain
Licensed under Creative Commons, Source.
The ACA supplies the medial and superior portions of the frontal lobe and the anterior parietal lobe, including:
- Pre-frontal cortex (executive functions - personality, decision making, planning, organisation), Supplementary motor area (changing between motor behaviours, role in speech production, micturition)
- Paracentral lobule (primary motor and sensory cortex corresponding to contralateral lower limb (medial homunculus) and continence).
- Corpus callosum
Blockage to the ACA will result in the following symptoms:
Executive Dysfunction
Executive dysfunction is an umbrella term that describes cognitive, behavioural and emotional difficulties that occur as a symptom of another disorder, in this case a stroke. Examples of executive dysfunction in ACA infarctions are shown below:
Apraxia
Apraxia is the inability to co-ordinate motor planning, meaning that simple motor tasks become very difficult. This presents with patients being unable to perform tasks like picking up a drink to take a sip despite knowing how to do it and having been able to do it in the past.
The regions of the brain that perform this function are usually found in the dominant hemisphere (usually the left hemisphere), which means that only ACA infarctions in the dominant hemisphere (usually the left hemisphere, but could be the right) will present with apraxia.
Dysarthria
Slurred speech is also common in ACA infarcts.
Personality Changes
Personality changes are also common in ACA infarctions due to damage to the frontal lobe. This is often noticed in the long term only, as in the acute phase the stress of the situation can mask a lot of personality changes.
Unilateral, Contralateral Motor Weakness in the Leg / Shoulder
The ACA supplies the medial portion of the brain, which includes the regions of the motor cortex that predominantly supply the contralateral leg and trunk (according to the motor homunculus).
The weakness will be contralateral to the side of the ischaemia as the motor impulses decussate (cross the midline) on their path from brain to muscle.
Unilateral, Contralateral Sensory Loss in the Leg / Shoulder
The ACA supplies the medial portion of the brain, which includes the regions of the sensory cortex that predominantly supply the contralateral leg and trunk (according to the sensory homunculus).
The sensory loss will be contralateral to the side of the ischaemia as the sensory impulses decussate (cross the midline) on their path from skin to brain.
Urinary Incontinence
The paracentral lobules are key for the control of micturition, and are made up of portions of the frontal and parietal lobes in the great longitudinal fissure (the middle bit between the two hemispheres of the brain). This midline portion of the brain is supplied by the ACA, so ischaemia in this region can lead to incontinence.
Corpus Callosum Involvement
The corpus callosum is supplied by the ACA, and this means that there is the potential for complex brain syndromes such as Alien Hand Syndrome and Split Brain Syndrome to occur with an infarction of the ACA. These syndromes result from the loss of the pathways through the corpus callosum, meaning the connections between the two hemispheres of the brain are significantly reduced or lost entirely. These are rare conditions.
The MCA supplies part of the frontal lobe, and the lateral parts of the temporal and parietal lobes.
The MCA has four main branches (lenticulostriate, superior, inferior and superficial). They all supply different portions of the MCA territory, meaning that a main trunk blockage of the MCA will take out all of them, and a small infarct may spare some regions. It is not important at this level to know which branches of the MCA supply which exact function.
The MCA supplies:
- Basal ganglia (motor control)
- Internal capsule (descending motor tracts)
- Lateral parts of the primary motor and sensory cortex (face, hand and arm)
- Broca’s area in the dominant hemisphere - responsible for the production of speech
- Wernicke’s area in the dominant hemisphere - responsible for the comprehension of speech
- The optic radiations
The MCA supplies a large area of the brain, meaning that a main trunk occlusion results in the loss of a massive portion of the brain, and is therefore associated with a high mortality.
Main trunk MCA infarctions are also prone to haemorrhagic transformation of an initially ischaemic injury, where the main trunk of the MCA is blocked and as the tissue dies, a bleed forms.
A blockage in the MCA may result in:
Unilateral, Contralateral Motor Weakness in the Face / Hand / Arm
The MCA supplies the lateral portion of the brain, which includes the regions of the motor cortex that supply the face, hand, and arm (according to the motor homunculus).
The weakness will be contralateral to the side of the ischaemia as the motor impulses decussate (cross the midline) on their path from brain to muscle.
However, in some MCA infarctions (depending on where along the path of the MCA the infarction occurs) a full hemiparesis may be seen, including the leg and shoulder, territories supplied by the ACA not the MCA. This is due to the loss of the internal capsule, which is the common path for all motor impulses leaving the primary motor cortex.
Unilateral, Contralateral Sensory Loss in the Face / Hand / Arm
The MCA supplies the lateral portion of the brain, which includes the regions of the sensory cortex that supply the face, hand and arm (according to the sensory homunculus).
The sensory loss will be contralateral to the side of the ischaemia as the sensory impulses decussate (cross the midline) on their path from skin to brain.
Contralateral Homonymous Hemianopia
Loss of the blood supply to the optic tract results in a homonymous hemianopia - this is a loss of one half of the vision on the same side of each visual field. The side of the visual field lost will be contralateral to the side of the lesion.
The hemianopia demarcation will be exactly down the midline of the vision - this is because all impulses that are traveling down the optic tract are lost.
For more information explaining the presentations and pathophysiology of visual lesions, please see our article here.
Aphasia
MCA infarction can lead to three different types of aphasia depending on which areas are damaged. However, aphasia only occurs if the dominant hemisphere is damaged, as both speech and language centres are found in the dominant hemisphere.
Broca’s Aphasia occurs when the Broca’s area of the dominant hemisphere of the brain is damaged. Broca’s area is located in the frontal lobe, and loss of function results in reduced speech fluency with preserved comprehension of the speech of others. It requires a lot of effort to produce speech, which consists of a few short words without sentence structure. Broca’s aphasia is also known as expressive aphasia.
Wernicke’s Aphasia occurs when the Wernicke’s area of the dominant hemisphere of the brain is damaged. Wernicke’s area is located in the temporo-parietal region, and loss of function results in fluid sentences composed of muddled words. It is often described as ‘word salad’ because the patient uses many words in sentences that are unrelated to the question, and so can also be called fluent aphasia.
Global Aphasia occurs when both Broca’s and Wernicke’s areas are damaged. This leads to the production of very few words that are not related to what the patient is trying to say.
Hemispatial Neglect
Hemispatial neglect occurs with a non-dominant hemisphere infarction of the MCA. It is a condition in which the patient is not able to acknowledge one entire half of their world despite the fact that they are physically able to see it. It is a loss of attention and awareness to one side of their world, and usually occurs on the contralateral side to the infarction.
It can lead to examples such as those below when the patient can follow instructions, but is only aware of one half of the task.
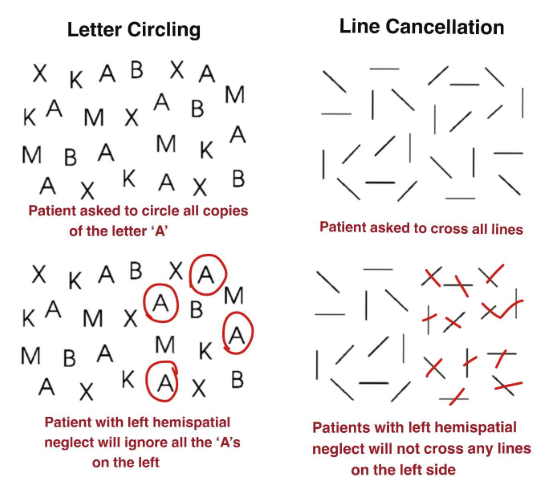
Diagram - Examples of Left Sided Hemispatial Neglect
Licensed under Creative Commons, Source.
The PCA supplies the occipital lobe (primary visual cortex), inferior temporal lobe and parts of the parietal lobe (including all optic radiations). It also supplies part of the thalamus (relay centre for tracts from cortex and body).
A blockage in the PCA may result in:
Contralateral Homonymous Hemianopia with Macula Sparing
The PCA supplies the primary visual cortex and the optic radiations. This means that a blockage in the PCA will result in a loss of one half of the vision, contralateral to the side of the lesion.
However, these lesions are often macular sparing because the macula (portion of the retina that receives images from the centre of the visual field) may have a dual blood supply from branches of the MCA and the PCA.
Contralateral and Complete Sensory Loss
The PCA supplies the thalamus, which is involved in the transmission of sensory impulses from the body to the cortex. A PCA infarction can therefore cause contralateral sensory loss, which is often partial rather than complete and depends on the specific thalamic nuclei affected.
There are many different arteries that supply the cerebellum, so any cerebellar infarction may involve the superior cerebellar artery, anterior inferior cerebellar artery or posterior inferior cerebellar artery.
An infarction in the cerebellum may result in:
Non-Specific Symptoms
Nausea, vomiting, headache, and dizziness can all be signs of cerebellar infarction, but are not enough to arouse suspicion with no other signs as they are so non-specific.
Sudden Onset Vertigo
Any patient with risk factors for a stroke presenting with sudden onset, unrelenting and position independent vertigo should be considered for a stroke as there are few other conditions that cause truly unrelenting, sudden onset vertigo. The key is a good history to differentiate other causes of vertigo such as Meniere’s Disease or acute labyrinthitis.
Ipsilateral Cerebellar Signs - DANISH
There are six symptoms that together represent the ‘cerebellar signs’ and suggest pathology in the cerebellum. Together they spell the mnemonic DANISH.
Dysdiadochokinesia - the inability to perform rapidly alternative muscle movements, such as rapid pronation and supination of one hand onto the other hand, or sliding the heel of one foot up and down the front of the other shin (called the heel-shin test).
Ataxia - a symptom characterised by a reduction in co-ordination and balance. It often results in a wide-based stance of walking, and can be confused with intoxication as the patient is unsteady and may stumble often on walking.
Nystagmus - nystagmus is an involuntary movement of one or both eyes with a rhythmic and repetitive pattern. The rhythmic movement is made up of a slow phase (which is the pathological deviation of the eye from where it’s supposed to be) and a quick phase (which is the snap back to where it should be to maintain vision). The eye or eyes can deviate in any direction (vertical, horizontal, rotational), and so all nystagmus should be investigated for an underlying cause like a cerebellar stroke.
Intention Tremor - an intention tremor is a tremor that is only present when trying to perform a task, and will not be present at rest. It is examined most often with the ‘finger-nose’ test, where the patient is asked to move their finger from their own nose to the examiner’s finger which is held in front of them. The tremor will be most prominent when the patient is concentrating to tap either their nose or the finger.
Slurred Speech - slurring of the speech is a sign of a cerebellar pathology. It is important when presented with a patient with slurring of the speech to check for other cerebellar signs or signs o0f cerebral ischaemia, as slurring of the speech can also be a sign of facial muscle paralysis as seen in an MCA blockage.
Hypotonia - reduced tone across the whole body is a sign of a cerebellar pathology.
Contralateral Ascending and Descending Tract Loss
All sensory and motor tracts travel through the brainstem on their way between brain and spinal cord. This means that a brainstem stroke will involve the loss of the sensory and motor impulses. These signs are often contralateral because many major sensory and motor pathways cross the midline at some point between the spinal cord and brainstem.
Ipsilateral Brainstem Signs
Brainstem signs are very complex, and you do not need to learn them in detail at this point. They share a common blood supply with the cerebellum, so some cerebellar strokes can cause brainstem signs.
The easiest signs to explain are the paralysis of cranial nerves; cranial nerves have nuclei in the brainstem, so the loss of blood supply to this will cause a paralysis of the nerve. This will occur on the same side, as the cranial nerves and nuclei do not cross the midline.
Basilar artery infarctions can cause sudden death, or can result in one of two syndromes depending on the location of the blockage.
If the blockage is at the distal end of the basilar artery, ‘Top of Basilar Syndrome’ occurs, resulting in:
- Visual and oculomotor defects
- Dreamlike behaviour, including an overly solemn demeanour
- Hallucinations
If the blockage is at the proximal end of the basilar artery, ‘Locked In Syndrome’ occurs, resulting in:
- Complete paralysis of all of the motor system
- Preservation of consciousness
- Preservation of vertical eye movements due to sparing of rostral midbrain structures above the level of the lesion
Locked In Syndrome therefore results in a patient that is completely aware of their situation but is unable to move their body except for vertical eye movement.
Bamford / Oxford Classification
The most commonly used classification system for ischaemic strokes is the Bamford or Oxford classification, and this categorises ischaemic strokes based on their initial presenting symptoms without the need for imaging.
Total Anterior Circulation Stroke (TACS)
A TACS is a large stroke affecting a large proportion of the cortex supplied by the anterior circulation.
It needs all three of the following symptoms:
- Unilateral weakness (and / or sensory deficit) of the face, arms or leg
- Homonymous hemianopia
- Higher cerebral dysfunction (such as dysphasia)
Partial Anterior Cerebral Stroke (PACS)
A PACS is a less severe form of a TACS where only a portion of the area supplied by the anterior circulation is affected.
It requires either two of the following symptoms, or isolated higher cerebral dysfunction:
- Unilateral weakness (and / or sensory deficit) of the face, arms or leg
- Homonymous hemianopia
- Higher cerebral dysfunction (such as dysphasia)
Posterior Circulation Stroke (POCS)
A POCS is a stroke involving a portion of the posterior circulation. It includes areas of the cortex supplied by the posterior cerebral arteries and infarctions of the brainstem and cerebellum.
It needs only one of the following (classical lacunar syndromes):
- Cranial nerve palsy and contralateral motor or sensory deficit
- Bilateral motor or sensory deficit
- Conjugate eye movement disorder (inability to move both eyes together in the vertical or horizontal plane).
- Cerebellar symptoms
- Isolated homonymous hemianopia with macula sparing
A LACS is a subcortical stroke, a blockage in one of the small branches known as the perforating arteries.
It needs only one of the following:
- Pure sensory deficit
- Pure motor deficit
- Mixed sensory and motor deficit
- Ataxic hemiparesis (weakness and ataxia present on the same side of the body).
Edited by: Dr. Marcus Judge
Reviewed by: Adrian Judge
In this article
A stroke is a life-threatening medical event that occurs when the blood supply to the brain is interrupted.
- 775

{kind=link}
{kind=link}