

Next Lesson - Development of the Urinary System
Core
Introduction
The urinary tract has four functional zones: the kidneys (filtration), the ureters (transport), the bladder (storage) and the urethra (voiding), and a single anatomical theme: a smooth-muscle wall lined by an epithelium specialised for urine. Knowing where each segment sits, how it is supplied and how it relates to neighbouring viscera is the foundation for understanding nearly every urological presentation, from a missed pyelonephritis to a postpartum stress incontinence.
This article gives the gross anatomy of each zone in order. The microscopic structure of the filtering unit is covered in The Nephron, the physiology of filtration in Glomerular Filtration Rate and the Measurement of Kidney Function, and the neural control of voiding in Micturition.
The Kidneys
Position and Surface Anatomy
The kidneys are paired bean-shaped organs lying in the retroperitoneum on the posterior abdominal wall. Each is approximately 11 cm long, 6 cm wide and 3 cm thick and weighs around 150 g. They lie obliquely against the psoas muscle, so their upper poles are closer to the midline than their lower poles.
The vertebral levels routinely tested are:
- Right kidney: upper pole at the level of T12, lower pole at L3.
- Left kidney: upper pole at T11, lower pole at L2-L3.
The right kidney sits about 1-2 cm lower than the left because the right lobe of the liver displaces it inferiorly. The hila of both kidneys lie at approximately the level of L1, the transpyloric plane.
Anteriorly, the kidneys are related to a stack of structures that vary between sides:
- Right kidney: liver (large area), duodenum (descending part), right colic flexure, small bowel and the right adrenal gland.
- Left kidney: stomach, spleen, pancreas (body and tail), left colic flexure, jejunum and the left adrenal gland.
Posteriorly, both kidneys lie against the diaphragm superiorly and the psoas major, quadratus lumborum and transversus abdominis muscles inferiorly. The 12th rib crosses the posterior surface of each kidney; the upper pole therefore lies behind the pleura, which is clinically relevant for percutaneous renal procedures and for blunt trauma.
Coverings of the Kidney
Each kidney is wrapped in three concentric layers, important for understanding both surgical access and pathology:
- Renal capsule: a tough fibrous coat directly applied to the kidney. It is non-distensible, which is why parenchymal swelling (e.g. acute pyelonephritis) produces flank pain.
- Perirenal fat (perinephric fat): a continuous layer of adipose tissue surrounding the capsule. The renal artery, vein and ureter run within it at the hilum.
- Renal fascia (Gerota's fascia): a fibrous envelope enclosing the perirenal fat and the adrenal gland. It is open inferiorly along the line of the ureter, so a perinephric collection can track down into the pelvis.
External to the renal fascia is the pararenal fat, which fills the renal angle and is the layer surgeons enter through a posterior lumbar approach.
Internal Structure
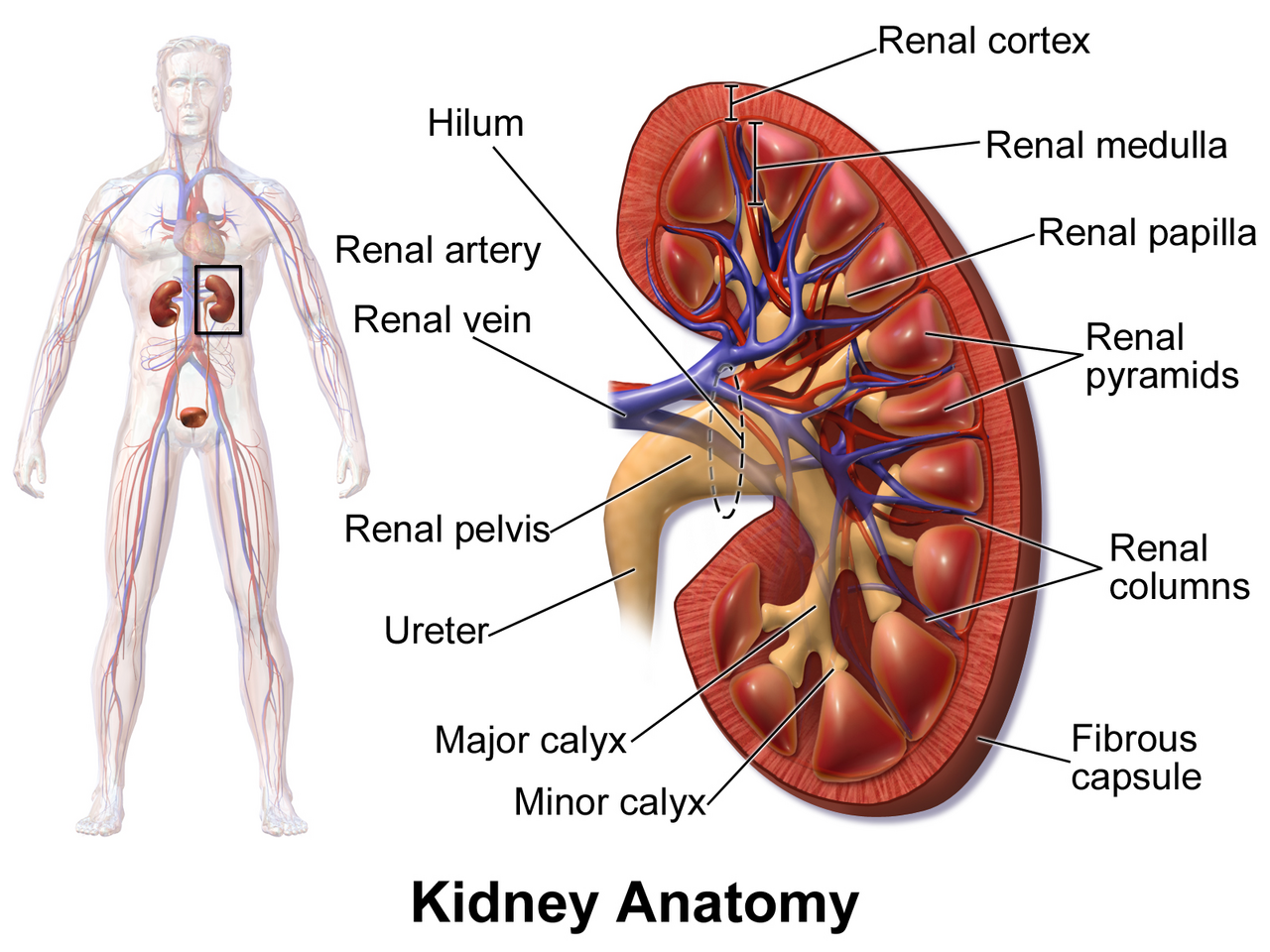
Diagram: coronal section of the kidney showing the outer cortex, the medullary pyramids, the minor and major calyces converging on the renal pelvis, the renal artery and vein at the hilum, and the ureter.
Creative commons source by BruceBlaus, CC BY 3.0.
On longitudinal section, the kidney has two clearly distinguishable zones:
- The cortex, the outer, paler region containing the glomeruli, proximal and distal convoluted tubules, and the cortical collecting ducts.
- The medulla, the inner, darker region organised into 8-12 cone-shaped renal pyramids. The base of each pyramid faces the cortex; the apex (the papilla) projects into a minor calyx.
Cortical tissue extends down between the pyramids as the renal columns (of Bertin). A lobe of the kidney is one pyramid plus its overlying cortex; an adult kidney typically has eight to ten lobes.
The collecting system is a series of progressively larger funnels:
- Minor calyces (8-12) receive urine from the papillae.
- Major calyces (typically 2-3) drain groups of minor calyces.
- The major calyces converge into the renal pelvis, a flattened funnel that exits the hilum.
- The renal pelvis narrows abruptly at the pelvi-ureteric junction (PUJ) to become the ureter.
Blood Supply
The kidneys receive about 20-25% of the resting cardiac output, far in excess of their oxygen demand: this reflects their role as filtration organs rather than tissues with high metabolic need.
Each kidney is supplied by a single renal artery, arising from the abdominal aorta at L1-L2, just below the origin of the superior mesenteric artery. Two practical points:
- The right renal artery is longer than the left because it must cross the midline behind the inferior vena cava.
- An accessory renal artery is present in around 25% of people, usually arising from the aorta and entering the lower pole. It is significant in renal transplant donor surgery and in some causes of secondary hypertension.
Inside the kidney the artery branches in a stereotyped sequence: renal → segmental → interlobar → arcuate → interlobular (cortical radiate) → afferent arteriole → glomerulus. The afferent arteriole is the resistance vessel that controls glomerular capillary pressure; this anatomy is the basis for the haemodynamic effects of ACE inhibitors and ARBs.
From the glomerulus, blood enters the efferent arteriole, a second resistance vessel. The cortical efferents form the peritubular capillaries surrounding the proximal and distal tubules; the juxtamedullary efferents continue as the vasa recta, long hairpin loops that descend into the medulla and are essential for the counter-current mechanism that concentrates urine. The vasa recta are described in detail in Control of Plasma Osmolarity.
Venous drainage mirrors the arterial supply, with venules combining into interlobular, arcuate and interlobar veins, then a single renal vein draining into the inferior vena cava (IVC). The left renal vein is longer than the right because the IVC sits on the right of the midline. It passes anterior to the aorta and is crossed by the superior mesenteric artery (SMA); compression between the SMA and the aorta is the cause of the rare nutcracker syndrome. The left renal vein also receives the left adrenal, left gonadal and left phrenic veins, whereas on the right these drain directly into the IVC.
Lymphatic Drainage and Innervation
Lymph from the kidney drains to the lateral aortic (para-aortic) nodes at the level of the renal hilum.
The kidney is innervated by autonomic fibres from the renal plexus. The dominant input is sympathetic from T10-L1 (via the lesser, least and lumbar splanchnic nerves), with a small contribution from the vagus. Sympathetic activity constricts the afferent arteriole, reducing renal blood flow and contributing to the renal response to haemodynamic shock. Sensory afferents travel back along the same routes; renal pain is therefore referred to the flank, T10-L1 dermatomes, and may radiate to the groin as the ureter is followed inferiorly.
The Ureters
The ureters are paired muscular tubes about 25-30 cm long that propel urine from the renal pelvis to the bladder by peristalsis. The wall has three layers: an inner mucosa lined by urothelium, a middle muscular layer (an inner longitudinal and an outer circular coat in the upper two-thirds, with an additional outer longitudinal coat in the lower third) and an outer adventitia.
Each ureter has an abdominal and a pelvic course. The abdominal ureter descends in the retroperitoneum on the medial border of psoas major, anterior to the tips of the lumbar transverse processes. It crosses the genitofemoral nerve and the gonadal vessels, then the bifurcation of the common iliac artery at the pelvic brim: this bifurcation is a useful surgical landmark. The pelvic ureter passes inferiorly and medially along the lateral pelvic wall, then turns anteromedially to enter the bladder at the vesico-ureteric junction.
The relationship of the ureter to other pelvic structures is sex-specific and clinically important:
- In the male, the ductus (vas) deferens crosses the ureter superiorly and medially as the duct passes from the deep inguinal ring towards the seminal vesicle.
- In the female, the uterine artery passes anterior (above) to the ureter just lateral to the cervix: "water (the ureter) under the bridge (the uterine artery)". The ureter is at risk of injury during hysterectomy at this point.
The classical teaching point is the three anatomical constrictions where renal stones impact:
- The pelvi-ureteric junction (PUJ).
- The pelvic brim, where the ureter crosses the iliac vessels.
- The vesico-ureteric junction (VUJ), the narrowest point of the entire urinary tract.
Blood supply is segmental and tortuous: the upper third by branches of the renal artery, the middle third by branches of the gonadal and common iliac arteries, and the lower third by branches of the internal iliac artery (vesical, uterine, vaginal, middle rectal). This poor anastomotic supply explains the sensitivity of the ureter to surgical devascularisation. Pain from a ureteric stone follows the dermatomes T11-L2 and is classically described as "loin to groin" colic, intense and intermittent.
The Bladder
Position and Peritoneal Relations
The bladder is a muscular reservoir for urine. In adults it lies in the true pelvis, posterior to the pubic symphysis, when empty; as it fills it rises into the abdomen and can be palpated above the pubic symphysis when it contains roughly 300 mL or more. In infants the bladder is an entirely abdominal organ, descending into the pelvis only during childhood.
The bladder has four surfaces:
- The superior surface: covered by peritoneum, in contact with sigmoid colon and ileum (and, in the female, the body of the uterus).
- Two inferolateral surfaces: against the levator ani and obturator internus muscles.
- The posterior surface (base): in the male related to the rectum (separated by the rectovesical pouch superiorly and the seminal vesicles and ductus deferens inferiorly), in the female related to the cervix and upper vagina.
The apex of the bladder lies anteriorly and is connected to the umbilicus by the median umbilical ligament, the obliterated remnant of the embryological urachus. The neck of the bladder is the most inferior point and is anchored by the puboprostatic ligaments (male) or pubovesical ligaments (female).
Internal Structure
The bladder wall has four layers:
- A mucosa lined by urothelium (transitional epithelium), which can stretch from a multilayered cuboidal arrangement when empty to a flattened squamous-like layer when full, all without losing its barrier function.
- A submucosa.
- A thick three-layered detrusor muscle, the smooth-muscle generator of voiding contraction. The detrusor is innervated by parasympathetic M3 muscarinic receptors: the basis for anti-muscarinic therapy in urinary incontinence.
- An outer adventitia (or peritoneum on the superior surface).
The internal surface of the bladder has two distinct regions:
- The trigone: a smooth, fixed triangular area at the base of the bladder bounded by the two ureteric orifices superolaterally and the internal urethral orifice inferiorly. It is derived embryologically from the mesonephric ducts (mesoderm), whereas the rest of the bladder is endodermal in origin.
- The remainder of the bladder: folded into rugae when empty.
The ureters pierce the bladder wall obliquely, traversing about 1.5 cm of muscle before opening at the trigone. This oblique course creates a flap-valve mechanism that prevents reflux of urine up the ureter when the bladder contracts. Failure of this mechanism causes vesico-ureteric reflux, a major cause of recurrent pyelonephritis and chronic kidney disease in children.
At the bladder neck, the smooth muscle thickens to form the internal urethral sphincter (sympathetic, α1-adrenoceptor-driven). Below this lies the external urethral sphincter, formed by skeletal muscle of the pelvic floor and under voluntary control via the pudendal nerve. The two-sphincter arrangement is essential for continence and is described in detail in Micturition.
Blood Supply, Lymphatics and Innervation
Arterial supply is from the superior and inferior vesical arteries, branches of the internal iliac artery. Additional small branches come from the obturator and inferior gluteal arteries; in the female, vaginal and uterine arteries also contribute.
Venous drainage is through the vesical venous plexus, which drains to the internal iliac veins. In the male this plexus is continuous with the prostatic venous plexus, providing one of the routes by which prostate cancer spreads to the lumbar vertebrae through the valveless Batson plexus.
Lymphatics drain to the external iliac, internal iliac and obturator nodes.
Innervation is autonomic and somatic:
- Parasympathetic fibres from S2-S4 (pelvic splanchnic nerves) cause detrusor contraction and internal urethral sphincter relaxation; the voiding response.
- Sympathetic fibres from T10-L2 (via the hypogastric plexus) inhibit the detrusor and contract the internal urethral sphincter; promoting filling and continence.
- Somatic fibres from the pudendal nerve (S2-S4) supply the external urethral sphincter for voluntary continence.
Sensory fibres carrying bladder fullness travel with the parasympathetics to S2-S4; pain fibres from the bladder dome travel with the sympathetics to T10-L2 and refer pain to the suprapubic region or lower abdomen, while pain from the trigone refers to the perineum.
The Urethra
Male Urethra
The male urethra is approximately 18-20 cm long and serves both urinary and reproductive functions. It is conventionally divided into four parts, in proximal-to-distal order:
- The pre-prostatic urethra (1-2 cm): from the internal urethral orifice through the bladder neck. The smooth muscle here forms the internal urethral sphincter, important during ejaculation to prevent retrograde flow into the bladder.
- The prostatic urethra (3-4 cm): passes through the prostate. On its posterior wall is a midline ridge, the urethral crest, which carries the openings of the prostatic ducts and, on a small mound called the verumontanum, the openings of the ejaculatory ducts and the prostatic utricle.
- The membranous urethra (1-2 cm): the shortest and least distensible segment, passing through the pelvic floor and surrounded by the external urethral sphincter (skeletal muscle, pudendal nerve). Its position deep within the pelvic floor means it is the segment most often torn in pelvic fractures. By contrast, the bulbar (proximal spongy) urethra is the segment classically injured by straddle trauma, where the perineum is forced against the inferior pubic ramus.
- The spongy (penile) urethra (about 15 cm): runs through the corpus spongiosum to the external urethral meatus. It receives the openings of the bulbourethral (Cowper’s) glands in the bulb and contains the small mucous urethral glands of Littré.
The male urethra also has two anatomical curves when the penis is dependent: a fixed proximal curve through the pelvic floor and a more distal curve at the base of the penis. This anatomy explains why catheterisation in men is technically more difficult than in women.
It also has three functional narrowings: the internal urethral orifice, the membranous urethra and the external urethral meatus, with the meatus usually the narrowest.
Female Urethra
The female urethra is approximately 4 cm long and 6 mm in diameter, running from the internal urethral orifice at the bladder neck, anteroinferiorly through the pelvic floor, to open at the external urethral meatus in the vestibule, just anterior to the vaginal orifice and posterior to the clitoris. It has only urinary function.
It is surrounded near its inferior end by the external urethral sphincter (skeletal muscle, pudendal nerve). Two pairs of small mucous glands: the paraurethral (Skene’s) glands: open into the urethra on either side of the meatus and are the female homologue of the prostate.
The shortness of the female urethra and its proximity to the vagina and anus account for the substantially higher rate of urinary tract infections in women. Stress urinary incontinence after childbirth is a separate issue and reflects damage to pelvic-floor support, the urethral sphincter complex and the levator ani.
The male urethra is supplied mainly by the inferior vesical and internal pudendal arteries (branches of the internal iliac), with the spongy segment also fed by the artery to the bulb of the penis. The female urethra is supplied principally by the internal pudendal and vaginal arteries. Lymph drains to the internal and external iliac nodes from the proximal urethra and to the superficial inguinal nodes from the distal portion (a useful staging point in urethral malignancy).
Clinical Correlations
A handful of clinical scenarios reinforce the anatomy:
- Renal stones (urolithiasis) impact at the three constrictions of the ureter (PUJ, pelvic brim, VUJ). Pain is "loin to groin", referred via T11-L2 dermatomes.
- Pyelonephritis stretches the renal capsule, producing the flank tenderness elicited at the renal angle: the angle between the 12th rib and the lateral border of erector spinae.
- Hydronephrosis: obstruction of the ureter or below causes back-pressure dilatation of the calyces and renal pelvis. The cause may be intrinsic (stone, tumour) or extrinsic (pregnancy, retroperitoneal mass, prostatic enlargement). See Urinary Tract Obstruction.
- Iatrogenic ureteric injury: classically during hysterectomy, where the ureter passes under the uterine artery 1-2 cm lateral to the cervix.
- Urinary retention in men: commonly caused by enlargement of the prostate compressing the prostatic urethra, since the urethra passes through the gland. Covered in Prostate Pathology.
- Catheterisation: in the male, lift the penis upwards to straighten the curves; in the female, the short urethra makes catheterisation generally easier but the close proximity of the meatus to the vaginal introitus is a source of error.
- Bladder rupture following blunt pelvic trauma is more common when the bladder is full and rises out of the protected pelvis; the dome ruptures into the peritoneal cavity, causing chemical peritonitis.
Summary
- The urinary tract is a continuous conduit from cortex to meatus, with each segment specialised for filtration, transport, storage or voiding.
- The kidneys lie in the retroperitoneum at T11-L3, wrapped in capsule, perirenal fat and Gerota's fascia. The right kidney sits lower than the left.
- The renal artery branches in a stereotyped order: segmental, interlobar, arcuate, interlobular: before reaching the afferent arteriole and the glomerulus.
- The ureters are 25-30 cm long, with three constrictions (PUJ, pelvic brim, VUJ) where stones impact. In the female the ureter passes under the uterine artery near the cervix.
- The bladder has a fixed trigone (mesoderm) and a rugose dome (endoderm). Detrusor M3 receptors mediate voiding contraction; the internal sphincter is α1-adrenergic and the external sphincter is somatic via the pudendal nerve.
- The male urethra is 18-20 cm with four parts; the female urethra is 4 cm. The length difference accounts for the markedly different burden of urinary tract infection between the sexes.
Reviewed by: Dr. Marcus Judge
In this article
The urinary tract is a continuous system from the renal cortex , where urine is formed, to the external urethral meatus , where it is voided.
- 130

{kind=link}